

Half a century ago, researchers who worked for the pharmaceutical corporations valued the lives of preborn children. These scientists worked hard to avoid injuring them as they developed new drugs for a wide variety of purposes.
But times have radically changed.
Big Pharma now spends millions of dollars annually specifically for the purpose of developing drugs and devices that deliberately kill the preborn child as efficiently and as easily (to the mother) as possible.
One 1980s political cartoon showed researchers saying, “Our new drug kills unborn children! We’re ruined!” Now the same scientists say, “Our new drug kills unborn children! We’re rich!”
In the 1970s, Garrett Hardin and other population theorists dreamed of a “contraceptive” that would most likely take the form of an abortifacient pill.1
With RU-486 and the mifepristone/misoprostol drug combination, it seems that the anti-life genie has finally granted their unholy wish.
How Medical Abortion Works
The scientific name of the RU-486 pill is mifepristone, which is sold under the brand names Mifegyn, Mifeprix and Korlym. It imitates progesterone, the hormone that signals the uterus to become receptive to the newly conceived human being.

Progesterone is necessary for the continuation of a pregnancy. If its levels drop too low, a miscarriage is inevitable. Mifepristone takes advantage of this. It contains a progesterone impostor that “plugs in” to the progesterone receptors in the uterus but does not deliver the message that progesterone is supposed to transfer naturally. This type of hormone impostor is commonly labeled an “anti-hormone.”
Once mifepristone has occupied the progesterone receptors, the blastocyst (early developing human being) is denied attachment and simply starves for want of nutrients and oxygen. He or she is expelled after several days. This mechanism of action also works to kill preborn children in the first ten weeks of pregnancy. Although, abortion clinics exceed this limit regularly. Women on Waves, for example, says that women can self-administer mifepristone to 12 weeks of pregnancy, a very dangerous practice because mifepristone does not abort ectopic pregnancies.2
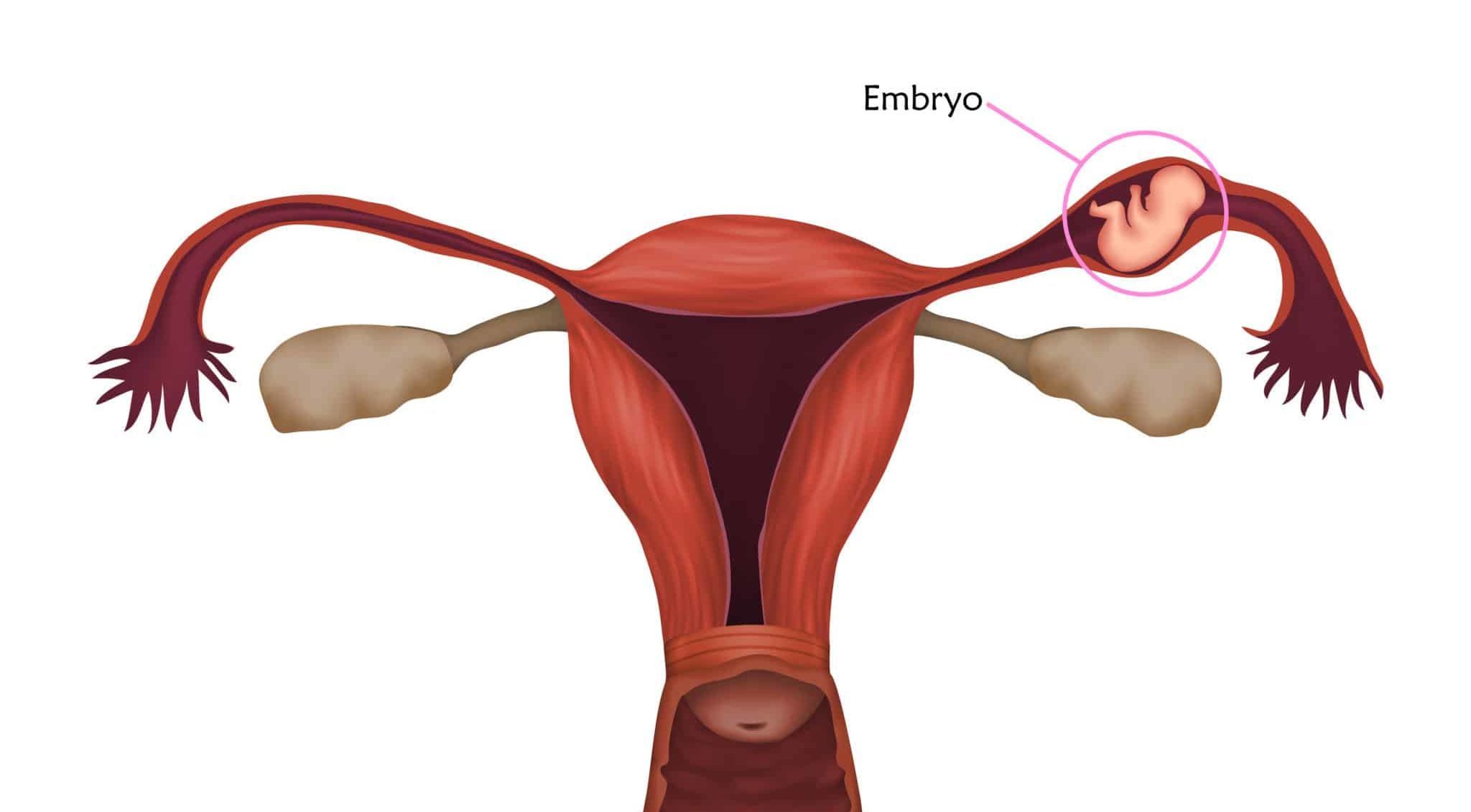
Illustration of an ectopic pregnancy
Mifepristone can be used alone but is only about 80 – 90% effective by itself. When used with a subsequent misoprostol pill, which causes the uterus to expel the preborn child, or with two injections of prostaglandin E or Sulprotone, it is about 95 – 97% effective at ending normal pregnancies.
However, it does not end ectopic pregnancies.
Misoprostol can also cause abortions by itself. In fact, many abortion pills are just pure misoprostol, often advertised under the brand name Cytotec.3 The chemical methotrexate is also a less effective single-drug option.
The third step in the medical abortion process is a follow-up appointment after about two weeks to make certain that the abortion is complete. They will use either an ultrasound or a blood test. However, these abortion clinics that do schedule this appointment for women report that many of them miss it. This means that about 3-5% will be surprised with a continuing pregnancy.
The entire three-visit mifepristone/misoprostol “medical abortion” regimen takes about two to three weeks. There have been nearly six million such abortions done since 2000.4
In fact, abortion pills accounted for more than half of all abortions in 2022.
Side Effects of Medical Abortion
The National Library of Medicine (NLM) Website contains the patient information pamphlets (PIPs) for every drug marketed in the United States for human and veterinary use.5
Few of these PIPs have a “black box” at the top, which reads:
WARNING: SERIOUS AND SOMETIMES FATAL INFECTIONS OR BLEEDING
Mifepristone is labeled with one of these “black boxes,” which are located right at the top of the patient information pamphlet. The January 2023 PIP by GenBioPro, available on the NLM Website, also includes a long list of side effects under Section 5, “Warnings and Precautions” and Sections 6, “Adverse Reactions,” including infection and sepsis (such as fatal septic shock), prolonged heavy bleeding (sometimes requiring a transfusion), missed ectopic pregnancy, anemia, immune system disorders, cardiac and vascular disorders, nausea, weakness, fever/chills, vomiting, headache, diarrhea, dizziness and even uterine rupture.
The April 2022 misoprostol PIP also features a “black box” which warns of the possibility of uterine rupture and birth defects if the medical abortion procedure fails. The list of side effects for misoprostol includes many of the same ones listed for mifepristone.
Surely, such a pill should not be taken alone at home, without the supervision of a doctor.
Abortion Pill Reversal
Medical abortion accounted for more than half of all abortions in 2022. Given the fact that hundreds of thousands of women now abort by pill annually, it is inevitable that some will have second thoughts after taking mifepristone, the first step.

Pro-life physicians have found that higher available levels of progesterone can override the effects of mifepristone and block its anti-hormonal action if administered early enough. In other words, progesterone can be an antidote to the poison of mifepristone. It’s more effective the earlier it is given after the mifepristone.
The latest that progesterone has blocked the action of mifepristone is three days.6 The general procedure is to inject the woman with progesterone for three consecutive days, then, every other day for two weeks, and then twice a week until the end of the first trimester.7 A progesterone supplement can also defeat the action of morning-after pills, which include other progesterone blockers like the ulipristal acetate in Ella.
As with any other pioneering surgical or medical procedure, the abortion pill reversal started out slowly and carefully. Drs. George Delgado and Mary Davenport were the first to attempt it and publish a study on it. Although the study sample was small, the results were promising. Four of six women who had taken mifepristone and then received the reversal delivered healthy babies normally. The other two miscarried, possibly due to the effect of the misoprostol they had taken.7
The experience of several other pro-life physicians is even more promising. Dr. Davenport has administered this reversal procedure to 106 women, and 56 have given birth to normal babies. More than 1,100 other pro-life OB-GYNs all over the world have begun to offer this service.8 OB-GYNs offering this reversal can be contacted here.
In 2019, an abortionist began a controlled study to determine the effectiveness of the abortion pill reversal. The study was conducted on women who had scheduled surgical abortions. First, these women were given mifepristone at 100 mg. 24 hours later, they took progesterone orally at 400 mg, twice daily, for three days. After three days, they continued to take progesterone once daily until their planned surgical abortion.
In the end, the study was ended early due to three patients hemorrhaging from the mifepristone. Thus, the official results of the study were inconclusive due to the dangers of the abortion pill. However, among the patients who received progesterone, 80% had a continuing pregnancy.
Heartbeat International has assumed the abortion pill reversal national network, and their hotline number is 877.558.0333.
Criticism of Abortion Pill Reversal
Not surprisingly, pro-abortionists have harshly – and unscientifically – criticized the pro-life physicians pioneering this procedure since its inception. The relentlessly anti-life American College of Obstetricians and Gynecologists (ACOG) has stated that abortion pill reversal is “unethical,” and has even claimed that “medication abortion ‘reversal’ is not supported by science.”9
However, Heartbeat International surveys of physicians who perform these procedures show that more than four thousand of them have been completely successful. In fact, several studies have shown that, once an abortion pill reversal procedure has begun, it has a 64-68% probability of resulting in a live birth.8
The most vocal critic of APR is Dr. Daniel Grossman. He was quoted in several mainstream media articles saying that the report was “very incomplete” and that it “hasn’t even been proven effective.”10 These media articles all mentioned that Grossman is an OB-GYN and a member of the American College of Obstetricians and Gynecologists. Somehow, they failed to reveal that he has also held high positions in Ibis Reproductive Health and the Population Council, which are both population suppression and pro-abortion organizations.
He is also a regular spokesperson for pro-abortion and population control causes and has written journal articles with such evenhanded titles as “The Public Health Threat of Anti-Abortion Legislation.” Additionally, he is a leading supporter of dangerous webcam abortions, having written an article entitled “Effectiveness and Acceptability of Medical Abortion Provided through Telemedicine.”
Apparently, such innovations are legitimate for “pro-choice” doctors, even if they endanger the lives and welfare of women. But let a pro-life physician try something new and lifesaving, and suddenly it is “unproven” and “potentially dangerous.”
The writers of these articles also did not bother to contact Dr. George Delgado, the pioneering researcher for this lifesaving treatment. One would think that, for the sake of completeness, the media would want to hear both sides of a potentially important story. This bias has always been particularly strong when the topic is abortion by pill.
At the very beginning of the battle over RU-486, a survey of more than two hundred magazine and newspaper articles found that only 9% mentioned any of the abortion pill’s numerous and serious complications or side effects. Only 8% quoted any pro-life experts or sources. And a lopsided 96% cast the abortion pill in a “very favorable” light. Marie Bass, former political director of NARAL and a major promoter of the abortion pill, said, “Press coverage really is good, if you think about it ― sometimes I worry that it’s almost too good.”11

Pro-lifers may wonder why Grossman and other pro-abortionists would be against women changing their minds ― in other words, having a choice. Perhaps this is one reason why their movement is now moving away from the “pro-choice” label and more openly supporting abortion as being a positive good for women and society.
Despite all of the propaganda to the contrary, experience has shown that pro-abortionists prefer to leave more control in the hands of physicians and less in the hands of women. Perhaps this is why they fail to condemn ― and, in some cases, even support ― atrocities. Examples include the Chinese forced abortion program and the decades of Indian forced sterilization camps which have victimized hundreds of thousands of women under filthy conditions.
This dichotomy is so extreme that three women professors wrote a book entitled RU 486: Misconceptions, Myths, and Morals, which describes how the abortion pill increases instead of decreases physician control and how it is dumped on third-world women in the developing world.12
In fact, the inventor of the RU-486 abortion pill, Étienne-Émile Baulieu, has said that the abortion pill provides “immense hope” for third-world women. These are the poor women who too often serve a dual role as guinea pigs and NGO-funded customers for contraceptives and abortifacients that are considered too risky for use by women in the United States.
However, it seems obvious that the main problem for Grossman and his supporters is that mifepristone reversals might make it appear as if some women actually do regret their abortion decision. This is a fatal blow to the popular pro-abortion propaganda. He said that “In my experience caring for women seeking abortion, they don’t go into this lightly. They’re very clear about their decision usually when they walk into the clinic and especially after they’ve gotten counseling … regret after an abortion is really rare.”8
Maybe ― and maybe not. But shouldn’t those women who do indeed regret their abortion decision ― regardless of how rare or how common they happen to be ― be empowered to reverse it?
Apparently not, in the opinion of Grossman and other pro-abortionists. For them, the only legitimate choice is abortion. In fact, abortionists sometimes exert extreme pressure on women to continue the abortion pill procedure even if their resolve has wavered after the first step. Women who have undergone successful mifepristone reversals have said Planned Parenthood personnel told them that, if they did not continue with the misoprostol follow-up, they would deliver deformed babies and suffer severe pain.
It remains to be seen if mifepristone reversal will continue on the road to becoming a commonly accepted medical practice. Pro-abortionists sometimes claim that a physician cannot be a competent OB-GYN unless they offer all available choices, including abortion. One can use this same logic the other way. If OB-GYNs (including abortionists) do not offer mifepristone reversals, they are not supporting the full range of possible choices themselves.
The Lethal Origins of RU-486
The tale of the abortion pill is laden with deception, outright lies, and dishonest manipulation of every kind.

The original manufacturer of the RU-486 abortion pill was the French company Groupe Roussel-Uclaf, a subsidiary of the West German pharmaceutical giant Hoechst. Hoechst had changed its name from the original “I.G. Farben” after World War II in an attempt to shake off its loathsome reputation. After all, the cyanide gas Zyklon-B, used by Nazis to exterminate Jews and others in the “showers” of their death camps, had proven very profitable to the company.
Now, I.G. Farben’s subsidiary is making an even greater profit by exterminating millions of preborn babies.
Ironically, the Pill’s inventor, Etienne-Emile Baulieu of France’s National Institute of Health and Medical Research, is Jewish. He was born in 1926 to Leon Blum and changed his name in 1942, perhaps to avoid being killed by the Zyklon-B gas made by the same company he worked for while developing the RU-486 pill.
On September 23, 1988, the French government, which just happened to own a little more than a third of Roussel’s stock, approved distribution of the abortion pill. But there were conditions. They approved it on the condition that it be administered only in approved medical centers and only until the seventh week of pregnancy. The manufacturer was immediately swamped with tens of thousands of pro-life protest letters, and more than 20,000 French pro-life activists marched in Paris streets in opposition to the Pill.13
For months, Dr. Edouard Sakiz, Roussel-Uclaf chairman, watched pickets outside his window at work. Pro-lifers publicly condemned his new product as “a chemical weapon that would poison the still-tiny children of a billion Third World mothers.” Jean-Marie Cardinal Lustiger, Archbishop of Paris, condemned the Pill as being “extremely dangerous,” both physically and morally.
On October 26, 1988, about one month after government approval of the Pill, Roussel-Uclaf suspended distribution in China and France. The “outcry of public opinion at home and abroad” was too much. Andre Ullman of Roussel-Uclaf, who helped develop the Pill, said that a boycott figured heavily in the company’s decision to stop making the drug.

Public Outcry
The backlash from pro-abortionists was incredibly vehement. As usual, it was short on science on long on hyperemotionalism. Faye Wattleton, then-president of the Planned Parenthood Federation of America, complained that the suspension was “a tragic display of cowardice and a shocking blow to women around the world.”14 Liberation, France’s largest left-wing daily newspaper, sneered at the Catholic Church in its front-page article entitled “The Diktat of the Bigots.”
The political weekly L’Evenement du Jeudi sniveled about “the brutal return of the Inquisition.” The French Family Planning Movement (including, of course, Planned Parenthood) trotted out its usual mix of tired slogans to condemn “…this new assault by conservative religious forces. … the traditionalists and Catholic reactionaries now want to impose their reactionary laws on women.”15
In response, on October 29, 1988, the French government ordered the company to resume distribution of RU-486. Health Minister Claude Evin, quoting France’s 1975 law legalizing abortion, stated that the Pill was “the moral property of the women of France.” Evin had invoked, for the very first time, a 1968 French law that allows the government to directly intervene when the “interests of public health” are endangered. Evin said, “I was doing what I could to make sure France did not surrender to pressure groups animated by archaic ideologies.”
Baulieu, the killer pill’s inventor, was now in the spotlight and parroted the usual pro-abortion lies. He said, “One hundred and fifty thousand women die annually from botched abortions. RU-486 could save the lives of thousands of women.”
Incredibly, pro-abortion groups even promoted Baulieu for a Nobel Prize nomination. It would be interesting indeed to see how the Nobel committee would justify elevating Baulieu to the same stature as Mother Teresa of Calcutta, who labored to save life rather than destroy it. She also condemned abortion during her own Nobel Prize acceptance lecture.
The invention of the abortion pill caused great excitement among pro-abortion groups in the United States. Several groups soon sprung up. These groups intended to spew propaganda to the public. Groups such as Every Child a Wanted Child (California) and the Reproductive Health Technologies Project (Washington, D.C.) were advocating for the Pill.
The intrinsic dishonesty of the pro-abortion movement was on full display as it worked hard to convince the public that the medical abortion pill was merely another contraceptive.

The public relations firm Bass and Howes developed and disseminated a neatly packaged and glossy press kit that included sample charts and graphs and photos. This press kit instructed the media to “emphasize the dearth of other contraceptive options available — particularly in comparison with what is available in other parts of the world” and “emphasize the issues of privacy, ease, safety, choice, and freedom, rather than of abortion and politics.”16
The Catholic Response
And a writer for the pro-abortion front group ‘Catholics’ for [a Free] Choice (CFFC) said:
If RU-486 is also used monthly, prolifers would have a hard time convincing the public that the drug isn’t just another contraceptive. Indeed, a 1982 New York Times story on Baulieu and RU-486 described the drug as “a new birth control pill.” Planned Parenthood released a “Fact Sheet” in October that refers to RU-486 as a type of “interceptor (luteal contraception).” If most people hear a new drug described as “birth control,” they’ll think of the Pill and IUD, not abortion…. If more women come to use RU-486 than traditional contraceptives, abortion would be the preferred method of birth control in the United States.17
The Archbishop of Lyon, Cardinal Albert Decourtray, summed up the feelings of pro-life Christians everywhere as he said, “The Pill now produces a process which allows abortion to seem like a contraceptive. In other words, it tends purely and simply to numb the conscience about both the act itself and its moral gravity. A follower of Christ cannot accept it.”
In November of 1988, the Holy See clarified its definition of abortion to include the use of drugs like the medical abortion pill, which are used specifically to kill the unborn child. Such use is an excommunicable offense for Catholics, the same as procuring a surgical ‘elective’ abortion.
International Responses
The United Nations World Health Organization (WHO) conducted detailed tests with the RU-486 pill and a similar drug, ZK 98.734, which was produced by Schering AG.18 It is obvious that WHO would have no particular interest in medical abortion unless the Pill would assist its population control programs. Baulieu himself has cited his own concern about the “complications of overpopulation” as one of the reasons he developed the abortion pill.19
The Population Council tested the medical abortion pill on 2,100 American women between October 1994 and December 1995. This trial deliberately excluded women over 35 years of age and those who smoked more than ten cigarettes each day. As a result, the Food and Drug Administration advises doctors to “treat these patients with caution,” and also to be very careful with women taking anticonvulsants or anticoagulants. On September 28, 2000, the FDA approved the RU-486 pill for use in the United States.

The Population Council gave the rights to produce the RU-486 pill to the New York-based marketing firm Danco Laboratories, which sells a chemical equivalent under the name Mifeprix or “Early Option.” The Shanghai-based Hua Lian Pharmaceutical Company makes the drug compound.20
Final Thoughts
Since the RU-486 medical abortion pill was approved for general use in the United States, nearly six million preborn children have lost their lives to it. Now, more than one-half of all abortions performed in the United States are non-surgical, or medical abortion by pill.4
This article was most recently updated in April 2023.
+ Endnotes
[1] Hardin, Garrett. “The History and Future of Birth Control.” Perspectives in Biology and Medicine, 1966.
[2] “How to Abort at Home with Pills (Misoprostol, Cytotec)?” Women on Waves. Accessed April 27, 2023. https://www.womenonwaves.org/en/page/702/how-to-do-an-abortion-with-pills–misoprostol–cytotec.
[3] Review of the National Institute for Health’s DailyMed Website, April 2022.
[4] Jones, Rachel K., et al. “Medication Abortion Now Accounts for More Than Half of All US Abortions.” The Guttmacher Institute, November 30, 2022. https://www.guttmacher.org/article/2022/02/medication-abortion-now-accounts-more-half-all-us-abortions.
[5] National Institute for Health’s DailyMed Website, which provides important information for every drug used in the United States on human beings or animals (veterinary use).
[6] Devine, Daniel James. “Cynthia’s Choice.” World Magazine, May 4, 2013.
[7] Delgado, George, M.D., and Mary Davenport, M.D. “Progesterone Use to Reverse the Effects of Mifepristone.” The Annals of Pharmacotherapy, December 2012.
[8] “Abortion Pill Reversal.” Home. Accessed April 27, 2023. https://www.abortionpillreversal.com/.
[9] “Medication Abortion Reversal Is Not Supported by Science.” ACOG. Accessed April 27, 2023. https://www.acog.org/advocacy/facts-are-important/medication-abortion-reversal-is-not-supported-by-science.
[10] Christie, Joel. “Pro-Life Clinic Now Offering ‘Abortion Reversals’ that Controversially Claim to Stop the Effects of the Termination Pill.” The Daily Mail, December 6, 2014. http://www.dailymail.co.uk/news/article-2863619/Pro-life-clinic-offering-abortion-reversals-controversially-claim-stop-effects-termination-pill.html.
[11] Grant, George. “Media Bias and Abortion.” Legacy, October 1991, page 1. Newsletter of Legacy Communications, Post Office Box 680365, Franklin, Tennessee 37068.
[12] Raymond, Janice, Renate Klein, and Lynette J. Dumble. RU 486: Misconceptions, Myths, and Morals. Institute of Women and Technology, c/o Room 3-405, Department of Urban Studies & Planning, Massachusetts Institute of Technology, Cambridge, Massachusetts 02139. 115 pages, 1991, 10.95.
[13] Geddes, Diana. “French Catholic Take a Beating on Abortion Pill.” National Catholic Register, November 13, 1988, page 1.
[14] Wattleton, Faye. Quoted in New York Woman, May 1990.
[15] Pomon, Dianne. “RU-486.” Voices for the Unborn. Feasterville, Pennsylvania, August 1990, pages 7 and 15.
[16] Grant, George. “Media Bias and Abortion.” Legacy, October 1991, page 1. Newsletter of Legacy Communications, Post Office Box 680365, Franklin, Tennessee 37068.
[17] Kaye, Tony. “Are You for RU-486?: A New Pill and the Abortion Debate.” Conscience [newsletter of ‘Catholics’ for a Free Choice (CFFC)], July/August 1986 [Volume VII, Number 4], pages 15-17.
[18] Batista, Joan. “Abortion Pill is No Panacea.” Against the Current, July/August 1990, pages 11-14.
[19] “RU-486: Major Topic at Conference.” WomenWise (newsletter of the New Hampshire Feminist Women’s Health Centers), 1986-1987.
[20] Zielinski, Lynne. “The Mother of All Pills.” Envoy Magazine [Volume 5, Issue 4], pages 48 to 51.





Dr. Brian Clowes has been HLI’s director of research since 1995 and is one of the most accomplished and respected intellectuals in the international pro-life movement. Best known as author of the most exhaustive pro-life informational resource volume The Facts of Life, and for his Pro-Life Basic Training Course, Brian is the author of nine books and over 500 scholarly and popular articles, and has traveled to 70 countries on six continents as a pro-life speaker, educator and trainer.
Marisa Cantu has a master's in political science and international affairs and a bachelor's in political science and has also studied international studies and French. She has a strong background in nonprofit work, research, writing, and policy proposal and analysis. She has written multiple articles on living the Catholic faith in everyday life, Catholic family life, devotions and prayers, and Catholic teachings.