

“Blessed are the wombs that never bore.”
The End of Generation
Sterilization is, in one sense, the epitome of anti-life activities, the crowning legacy of people like Margaret Sanger, Marie Stopes, and other eugenicists. This is because it fully achieves the end that those activists hoped for: removal of the generative capacities of human beings. Like neutering or spaying dogs, anti-lifers permanently destroy men’s and women’s reproductive organs in sterilization. The selling point is that it allows unregulated pleasure with absolutely no chance to beget new life. So, as a supposed permanent and absolute “alternative” to contraception, the purpose for most individuals who pursue sterilization is to allow pleasure without promise—no promise to bear life. However, the purpose of many ideologues who push sterilization around the world (especially in the Global South and developing countries of Africa and South/Southeast Asia) is more akin to eugenic population control, just like Sanger and Stopes originally intended.
With sterilization, fecundity is permanently canceled. Indeed, when Our Lord said that there would come days when they would call the barren blessed, He might have been thinking of our own time.
The topic of sterilization is broad. In this article, we will focus on technical and medical concerns for individuals who get sterilized. We will start with general facts about sterilization, then consider the methods, health effects, and other concerns involved with female sterilization and then male sterilization. But none of this should eclipse the main point about sterilization: it is inherently, unmitigatedly, grossly immoral. To destroy organs of the human body with the direct intention of ending the capacity to beget children is directly repugnant to the first commandment of the Creator: “Be fruitful and multiply” (Gen. 1:28).
Male and Female Sterilization: General Facts
There are two halves of the coin: female sterilization and male sterilization. The former has historically been more popular, although the latter is rising in popularity, and efforts to push it are increasing. As methods of so-called “family planning,” both kinds of sterilization are a major part of the global population control campaign that has been targeting Africa, South Asia, and other regions of the world for decades. To this end, sterilization is usefully marketed as “permanent contraception,” and it is often administered immediately after a woman gives birth, for example in places like Kenya.1 It is also administered after abortions.

What may be most surprising about sterilization is that it is the most popular kind of “contraception” (as far as it can be considered a kind of contraception) in the United States, and it is very popular in other developed countries. According to Contraceptive Technology, 21st Edition, the 2011-2013 National Survey of Family Growth found that 25.1% of contracepting couples used female sterilization, and 8.3% used male sterilization. That gives a whopping 33.4% of couples using sterilization as their “method of choice” to prevent new life in their sex acts, or 12.5 million people—all in the United States alone.
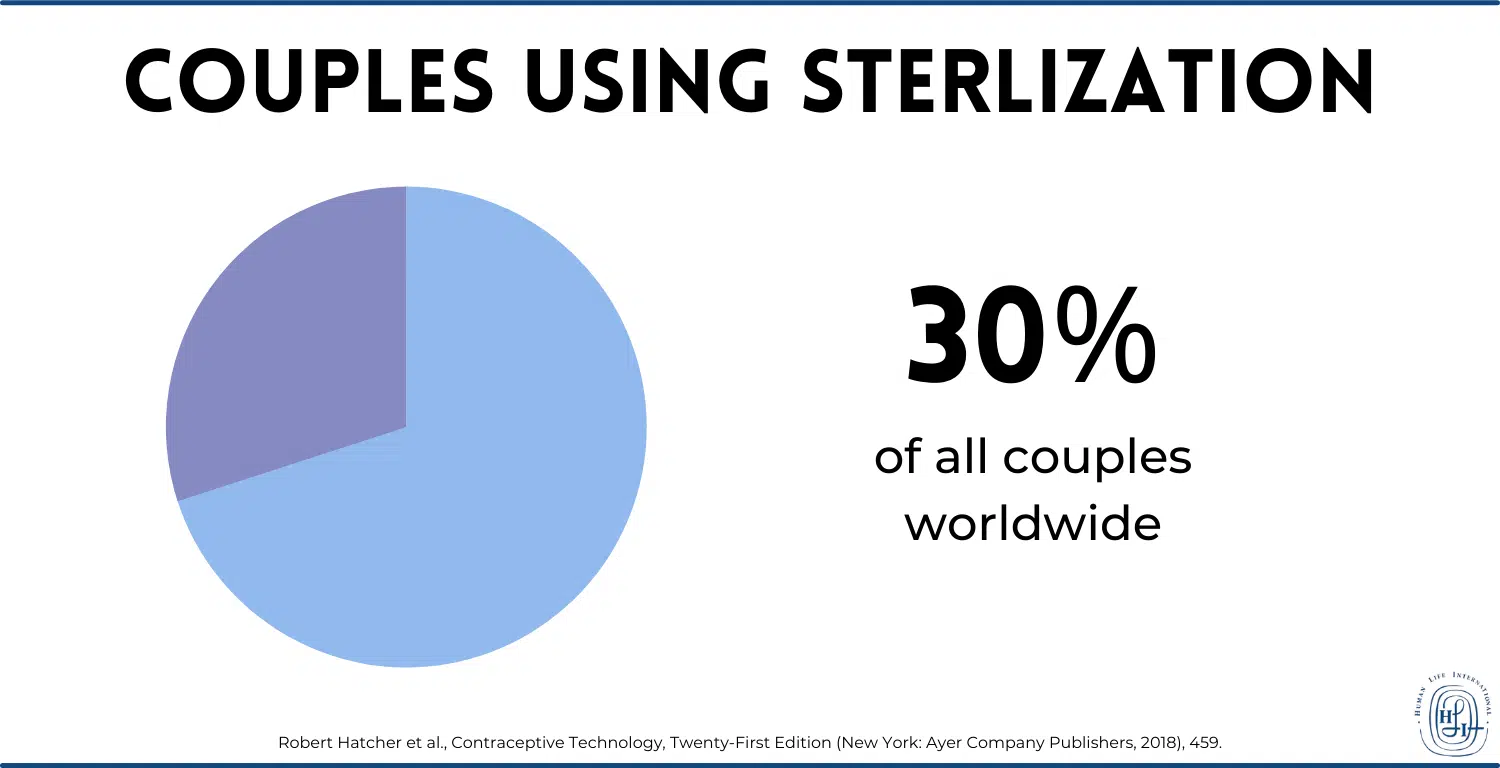
Around the world, more than 30% of all couples use sterilization.2
These are enormous numbers, and even though only 10% of couples in the developing world are sterilized, Western ideologues would love to increase that number, since they would prefer those populations to have the least chance of producing new life.
With all that said, we will move onto the specifics of the procedures and damages done to women’s and men’s bodies in sterilization. Fair warning: sterilization is one of the most disgusting anti-life phenomena to talk about, so readers should beware. We must discuss not only the moral depravity of sterilization, but also some specific health risks associated with the methods of female sterilization and male sterilization; this requires some gory details.
Female Sterilization (Tubal Occlusion, Ligation, or Removal)
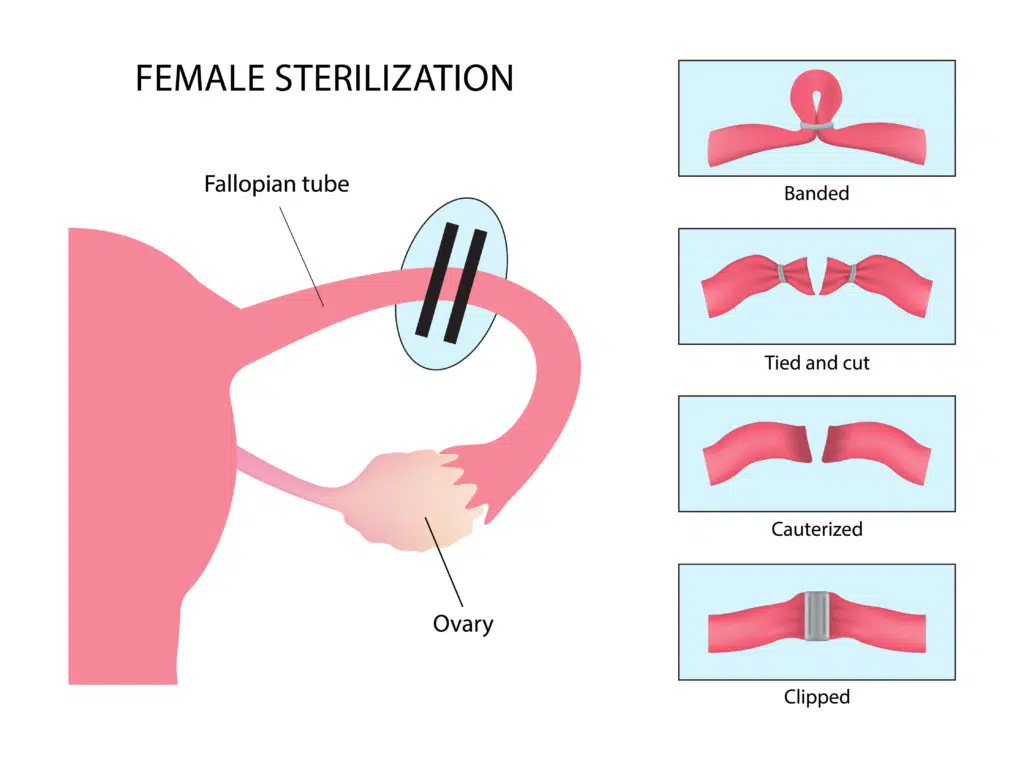
Historically, female sterilization has been more popular than male sterilization. Female sterilization basically consists of destroying or somehow preventing the function of the fallopian tubes, which carry eggs from the ovaries to the uterus. If the tube has been damaged or removed, then eggs can’t pass through the tubes, and sperm cannot reach them during intercourse. There are various forms of tubal ligation, occlusion, or removal, in which the fallopian tubes are tied, cut, clamped, or even blocked according to diverse and grotesque techniques. Let’s discuss them.
All of the following information comes from Contraceptive Technology, 21st Edition, from Chapter 16 on so-called “Permanent Contraception” (i.e. sterilization).
Most tubal ligation/occlusion procedures are performed by laparoscopy, where a camera is inserted into the pelvic cavities via small incisions. Using this format, the surgeon has many choices as to the method of destroying or maiming the woman’s fallopian tubes, including:
- Electrocoagulation – The surgeon uses electricity to burn and cauterize the fallopian tubes; tissue coagulates, blocking the passage of eggs.
- Mechanical clips and bands – The surgeon can place various name-brand clips, rings and bands, like the Falope Ring, the Ulka-Clemens clip, and the Filshie clip, to squeeze the fallopian tubes shut. The devices are made of metal, plastic, or silicone, and can have spring parts and interlocking teeth.
- Salpingectomy – Technically this method is neither tubal ligation nor occlusion, because instead of blocking or “tying” the tubes, the surgeon just cuts out the fallopian tubes entirely.
- Minilaparotomy – The surgeon makes incisions below the navel, and from there can either perform a partial salpingectomy (cutting away the middle of the fallopian tube and leaving behind some behind on the ovary side and the uterine side) or a full salpingectomy.
There is also the hysteroscopic approach, which inserts a camera through the cervix rather than through incisions in the abdomen. The only method available in the United States that uses the format is the Essure device, a metal coil inserted into the fallopian tubes. The device itself is meant to cause inflammation by embedding fibers into the wall of the fallopian tube, which will then develop inflamed tissue that eventually seals off the tube, after about three months.
Screenshot from the Essure Coil’s Instructions for Use
Health Effects of Tubal Sterilization
One of the consequences of allowing sharp instruments and metals inside one’s body in order to damage and destroy healthy organs is the range of potential side effects. Sterilization is inherently unhealthy, and the list of associated health risks is not short.
Menstrual Problems
Although menstrual problems are probably the least common health problems, some women do report them. There are not enough good randomized, controlled experiments on the subject to make any proper assertions (according to the authors of Contraceptive Technology), given that many women used hormonal contraceptives prior to being sterilized, and weight change and aging present confounding variables. But it seems to be the case that at least some women report menstrual problems, enough for there to be a named post-tubal ligation syndrome, although Contraceptive Technology doesn’t consider it definitive. Between 2% and 4% of patients in trials for Essure and Adiana (a different device, which is no longer in production) said they had menstrual disturbances following their procedures, which, again, some explain away by alluding to other possibilities.
What is known is that, at least subjectively, some women feel tubal sterilization affects their menstruation.
Surgical Complications
Laparoscopic surgery comes with the risk of bowel, bladder, and major vessel injuries. While these are not common, it is dependent on the conditions of the woman’s anatomy, including obesity, and the surgeon’s skill. But accidents can always happen; minor and major injuries are unpredictable and possible. Other complications, like the necessity for a blood transfusion and febrile morbidity (severe fever), occur 0.9% to 1.6% of the time. Contraceptive Technology also indicates the possibility of wound infection and prolonged pelvic pain. In hysteroscopic Essure placement, rupturing the tube occurs in 1% to 3% of cases. Infections, bleeding, and injury to other organs are also possible in hysteroscopic procedures.
Post-Ablation Tubal Sterilization Syndrome
In women who have received both tubal sterilization and endometrial ablation, or removal of the uterine lining (sometimes used to treat excessive uterine bleeding), the incidence of post-ablation tubal sterilization syndrome is 8% to 33%. The syndrome refers to the accumulation and distention of blood stuck in the cornua (where the fallopian tubes and the uterus meet) or the near end of the tube; the trapped blood causes significant pain. There is an increased risk for women who receive the Essure device and later need an endometrial ablation, because certain ablation procedures use radiofrequencies that can be conducted by the Essure’s steel core and damage other organs.
Chronic Pelvic Pain
As with menstrual dysfunction, reports of chronic pelvic pain are difficult to analyze statistically. However, they do exist, especially among younger patients who have had previous menstrual trouble. According to a study cited in Contraceptive Technology, after Essure placement, 8.1% of women may have pelvic pain, continuing in 4.2% of them after three months. However, these numbers grow; within a year of placement, 19.2% of women report pelvic pain, and after a year, 30.8% do. This number is likely to increase with time, and the risk of pain increases with previous history of pelvic pain.
Hysterectomy
It is unknown why, but there is a high risk of the need for a hysterectomy, or the removal of the uterus, in women who have had tubal sterilization surgery. They can be up to 4.4 times as likely to receive the procedure than those couples whose male member had a vasectomy. The probability of getting a hysterectomy after 14 years from being sterilized was found to be 17%, quite a high probability for such a rare procedure.
Ectopic Pregnancy
The most frightening risk of any kind of tubal ligation/occlusion or removal, but especially electrocoagulation, is ectopic pregnancy. This is a pregnancy where the fertilized ovum implants in the fallopian tube, rather than the uterine wall. It is usually fatal for the woman if left untreated, since the baby will grow in the wrong spot and rupture the woman’s abdomen. There have been extremely few cases of babies who survived and were born from an ectopic pregnancy.
Now, the purpose of sterilization is to sterilize and render pregnancy impossible; but new life can still arise at times (we’ll get to that in a bit). When it does, the risk that the resulting pregnancy is ectopic is very high, about 30%—15 to 20 times the rate for non-sterilized women.3 The total cumulative probabilities over ten years for ectopic pregnancy for each method of tubal sterilization are still low, around 1% or less. But for women under thirty, the probability is greater; it can triple to about 3% (31.9 per 1000 sterilizations) after electrocoagulation in particular.
Other Major Concerns with Tubal Ligation/Occlusion or Removal
The problems with tubal sterilization do not stop at moral and health concerns; there are also practical concerns as well. For instance, although female sterilization is supposed to be permanent, there is remote potential for the method not to succeed in preventing new conception. As we mentioned, when that happens, an ectopic pregnancy is likely. The various methods carry different probabilities, but the average rate is 0.5% pregnancy within a year after tubal sterilization. Over five years, the cumulative rate ranges from 0.5% to 1%, and that number increases the younger the woman is when she gets sterilized. As for the Essure device, estimated rates are higher, 0.5% in one year and 1% over ten years. However, “successful placement rates” (meaning the metal coils are stuffed securely into a woman’s tubes) range from 81% to 98%, meaning there is greater likelihood that the coils won’t even be placed properly to prevent conception.
There’s an even bigger problem with sterilization: women regret it. As reported in Contraceptive Technology:
- The cumulative fourteen-year probability of regret is 12.7%, or about one in eight women.
- Women who were younger than thirty when they had their “tubes tied” regretted with a probability of 20.3%; that’s more than one in five young women. Even the rate for women older than thirty when operated on was 5.9%, over one in twenty women.
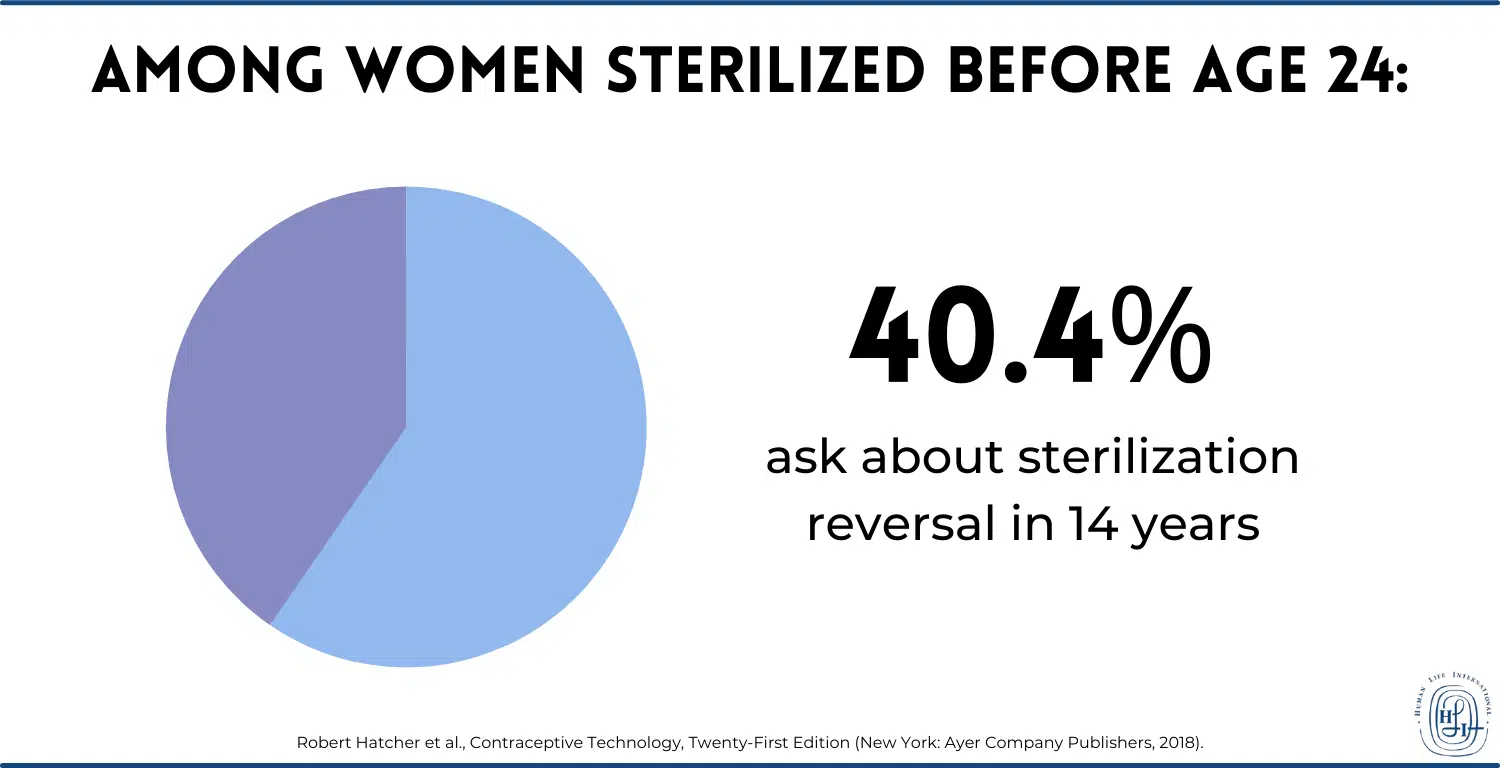
- And within the same fourteen-year period, the rate of women who ask for information about reversing sterilization is 14.3% (about one in seven women). For women who get sterilized before age 24, the number can be as high as 40.4%.
That’s too bad, because reversal is extremely impractical; there is a reason they call it “permanent contraception” in the anti-life arena. If you want to become pregnant after female sterilization, either you have to use in-vitro fertilization, itself highly immoral, and highly expensive, or you try to reverse the operation. The reversal depends very specifically on each case and the method of tubal sterilization employed, but all attempts to reverse carry risks. These include surgical mishaps, anesthetic accidents, and ectopic pregnancy rates between 4% and 8%.
Lastly, there are a few things to note about the Essure device, which carries with it special concerns. Soon after its introduction, increasing numbers of women began to request its removal, for all kinds of reasons. These included pregnancies, chronic pelvic pain, menstrual dysfunction, and nickel hypersensitivity (not to mention improper placement of the coil itself). In November 2016, Essure was required to have a black box warning about the myriad problems it has.

Now let’s take a look at the male counterpart to female sterilization: vas sterilization.
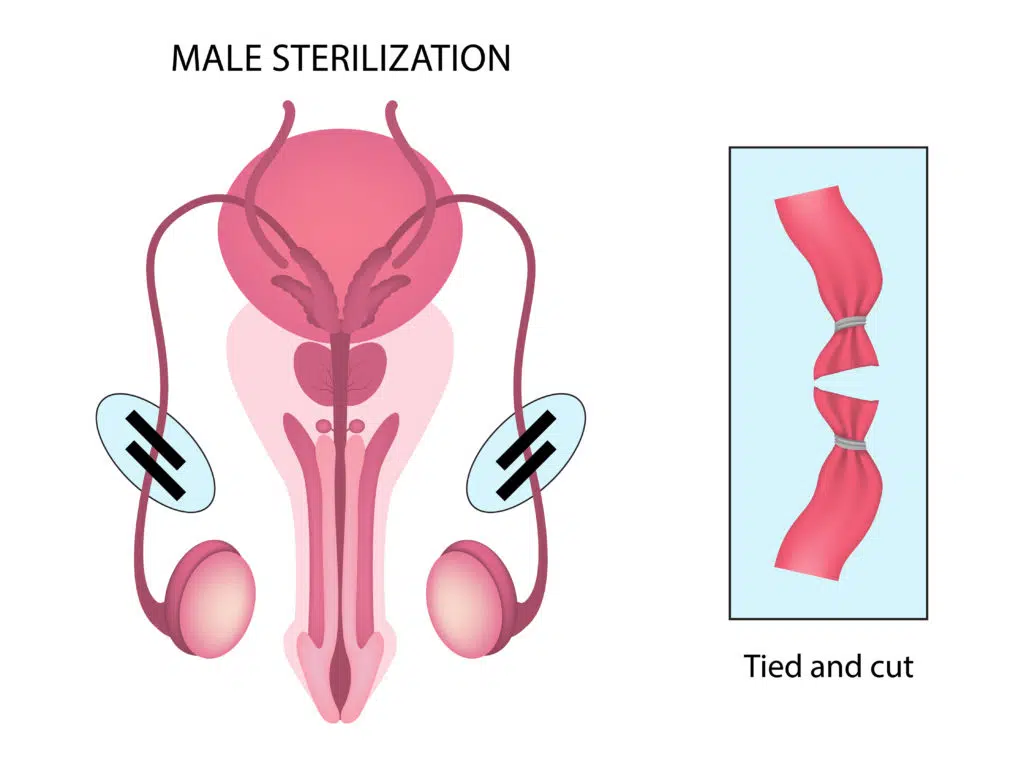
Male Sterilization (Vas Sterilization or Vasectomy)
The mechanism of male sterilization is the severing or otherwise blocking of the vasa deferentia (plural of vas deferens), which prevents them from transmitting sperm from the testes. As a result, semen will have no sperm in it, and intercourse will be sterile. The most common way to do this is to snip the tubes as a form of very precise castration, but there are also newer ways to obstruct these delicate tubes. As with tubal sterilization for women, the various methods of male sterilization are quite disgusting; we will cover them for completeness’s sake, and to see just how grotesque the whole business of sterilization is.
Again, all of this information is from the sixteenth chapter of the twenty-first edition of Contraceptive Technology.
The first step to destroying the function of the vasa is to isolate them; this can be done in a variety of ways. Conventional vasectomy is the oldest method, which uses 1.5- to 3-centimeter-long incisions in the scrotum, made with a scalpel and sewn shut by suture after the sterilization is done. The actual sterilization occurs when the vasa are cut and occluded using surgical scissors, and then the ends of the sliced tubes are occluded (using one of the methods described in the next paragraph). “No-scalpel vasectomy” was invented in 1974 by a Chinese doctor looking for a faster way to do this. First, a ring clamp is placed around the vas, perivasal tissue (tissue around the vas), and the skin of the scrotum. Then a special “vas dissector” is used to aid in grasping the vas, snipping it, and occluding the ends according to the various methods. Sutures are not used normally, since only a tiny incision is made. No-scalpel vasectomy is a type of so-called “minimally invasive vasectomy,” which includes various other technical variants of manipulating and maiming a man’s private parts.
After that, there are various methods of occluding or ligating or removing the vasa deferentia, including:
- Ligation – The surgeon ties up the tips of the snipped vasa deferentia using ligatures, removing about a centimeter from each vas between the tied ends.
- Clips – Similar to ligation, but the surgeon uses clips to clamp the sliced ends shut instead of ligatures.
- Thermal or electocautery – The surgeon uses electrical or thermal instruments to burn the mucosa around the snipped ends of each vas.
- Fascial interposition – The surgeon usually uses this method in addition to others; a layer of spermatic fascia, which is connective tissue nearby the vas, to add an extra barrier between one or both ends of the split vas.
- The Marie Stopes International technique – The surgeon uses electrocautery to burn and destroy two and a half to three centimeters of each vas; this method is the only one that does not involve division or excision of any part of the vasa. It is not used in the United States, but only in countries where MSI operates, many of which are poor developing countries.
There is also chemical occlusion, but this is a very uncommon method for humans.4 That’s just one more indication that sterilization is like neutering or spaying a dog.
Side Effects of Vas Sterilization
As with female sterilization, male sterilization carries with it a retinue of health detriments, stemming from the very fact that any kind of sterilization is directly contrary to health, which is the proper functioning of the body. It is inherently unhealthy, and that shows. While the list of potential side effects of male (vas) sterilization is slightly shorter than that of female (tubal) sterilization, it does not mean there is necessarily a smaller rate for some of them. Nor does it mean that they are any more pleasant.
Surgical Complications
While vasectomy is less invasive than tubal sterilization, there is always the possibility of complications, including severe ones. There can be injuries from slicing instruments, or the procedure can go awry in various ways:
- One particularly difficult possibility is that the same vas deferens is occluded in two places, rather than both vasa deferentia. This both invalidates the procedure and can cause more damage (that is, more than what the inherently damaging operation already does). It is a mistake made more likely by using a “single midline incision” in no-scalpel vasectomies (i.e. instead of two).
- Although there are only 0.5 deaths per hundred thousand men sterilized by vasectomy, 1% to 2% of men who get sterilized do form hematomas (bleeding inside of the scrotum) or get infections, regardless of the method used.
- Fournier’s gangrene, a condition in which flesh decays under a serious infection, has also been reported, though very rarely.
In general, while under 3% of vas sterilization procedures result in medical need, the list of possible complications, in addition to the above, can include: vasovagal reaction (slowing of the heart and blood flow that can result in faintness and more),5 lidocaine poisoning (too much anesthetic), bleeding, bruising, and swelling.
Chronic Scrotal Pain
One of the most unpleasant possible side effects of vasectomy is chronic scrotal pain, which afflicts between 1% to 2% of men who get sterilized. This pain can be severe, so much so that it has its own name: post-vasectomy pain syndrome. It can take months or years to show up, and when it does, it can become a continual health problem. While its source is unknown, speculation includes all manner of difficulties, from congestion of the occluded vasa, to explosion of the epididymis (the intermediate tube between the testicle and the vas deferens), to damage to the scrotal or spermatic cord nerves. In cases where regular treatment fails, surgery might be required, including various excisions, all the way to orchiectomy (removal of the testicals from within the scrotum).
Anti-Sperm Antibodies
One other special difficulty that comes from vas sterilization is the formation of anti-sperm antibodies. While only 8% to 21% of men in the general population have anti-sperm antibodies, an incredible 50% to 80% of sterilized men have them. While these antibodies, which kill sperm, are not otherwise dangerous to the body, they matter in two cases:
- Sterilization “failure” (i.e. regular operation of the reproductive system that results in pregnancy)
- A reversal attempt
With that, then, let’s move on to discuss these cases.
Other Major Concerns
While we shouldn’t consider impregnation a “failure” of a system designed to do just that, the male sterilization procedure, just like the female one, can still allow for pregnancy (meaning its anti-generation function isn’t foolproof). Vas sterilization generally will allow pregnancy 0.15% of the time (as opposed to 0.5% for tubal surgery), which makes it a more “effective” anti-generation method. But pregnancies still can happen. And the cumulative probabilities of pregnancy per 1000 vasectomies is: after one year, 7.4, and after two, three, and five years, 11.3.
But the real concern, as with female sterilization, is the possibility of regret. Permanently damaging himself and destroying his fertility is inherently a regrettable decision for a man. Rates of overall regret among men are 1% to 2%, which is lower than that of sterilized women. However, the women in men’s lives regret the vasectomy at rates of 6% to 8%. Like with tubal sterilization, the younger or more uncertain a man’s relationship future is, the higher the likelihood of regretting the permanent decision to neuter himself.

And that decision, again like tubal sterilization, really is essentially permanent. There are only two tenuous options after a vasectomy:
- In-vitro fertilization or other “assisted reproductive technologies”—in other words, expensive, artificial, and highly immoral technological parodies of intercourse
- An attempt at reversal, which involves extremely technical and advanced microsurgical skills on the part of the operator.
The second method’s impracticality makes sense when one considers that two tiny tubes have been sliced, blocked, tied, or otherwise maimed, and now they have to be reconnected. In addition, timing becomes a serious factor in an attempt at reversal. If a reversal attempt is performed within ten years after a vasectomy, rates are somewhat better; after that, rates of impregnations drop off to less than 50%. If a man wanted to get a woman pregnant, even after reversal, anti-sperm antibodies could have an enduring effect that likely hinders or altogether arrests the possibility of conception. In general, post-reversal pregnancy rates range from 38% to 89%, while IVF rates are 17% to 36%.
In short, “permanent contraception” describes vas sterilization accurately in the sense of permanence. Fair warning to men who would castrate themselves.
The “Choice” That Ends Choice
Everyone has the freedom to make medical choices that affect his or her health. However, many people are not aware of the damage that sterilization inflicts on their bodies in the long run. Others feel that the risks are outweighed by the seductive but false promises of freedom and security that sterilization offers in the short term.
The fact of the matter is that anyone who chooses sterilization is forced to accept hard realities:
- You are forced to accept risks to your health. The side effects of various medical procedures of tubal occlusion/ligation and vas surgery vary from minor inconveniences to fatal difficulties. All side effects are unpredictable. If you choose a sterilization procedure, you are exposed to health risks that you cannot predict or avoid and potentially cannot treat
- You can never change your mind. The moment you have a sterilization procedure, you give up choice in the matter forever. Although reversal procedures are possible, they are expensive and likely unsuccessful. You may even be led down a compoundedly immoral path by attempting IVF, which is gravely sinful, as well as expensive and not necessarily successful. For all intents and purposes, then, you will never have the option to bring forth a child if your circumstances or views change.
The end result is that sterilization, by inflicting severe damage to a body, removes a person’s control over both parental capability and health. It is simply and objectively the destruction of one’s reproductive organs. The medical advice that sterilization is a “safer choice” for “contraception” is contradictory, since the methods of sterilization inherently require administering damage to a previously healthy body and setting its future safety at serious risk. And furthermore, rather than protecting a person’s ability to lead a healthy life, they limit his or her options by permanently removing fertility, for all intents and purposes rendering him or her incapable of ever becoming a mother or a father.

Sterilization, rather than providing the promised freedom and safety, restricts a person to a condition of uncertain personal health and irreversible infertility. But the bottom line is that these natural problems are the reflection of supernatural problems. The reason sterilization and its consequences are so horrific to discuss is because they are morally egregious. Sterilization is certainly a mortal sin, and its practical permanence is one of the reasons it is worse than contraception. Not only is it intended to inhibit God’s life-giving intent for human sexuality simply for the purpose of lust, but it also directly destroys His creation, the male or female body.
We urge you to explore our other resources that discuss the beauty of human sexuality as God intended it: between one man and one woman, open to life, for all their life.
+ Endnotes
[1] Faith Kasiva, Robbed of Choice: Forced and Coerced Sterilization Experiences of Women Living with HIV in Kenya, edited by Jane Godia (African Gender and Media Initiative, 2012).
[2] Robert Hatcher et al., Contraceptive Technology, Twenty-First Edition (New York: Ayer Company Publishers, 2018), 459.
[3] Tyler Mummert and David M. Gnugnoli, “Ectopic Pregnancy,” StatPearls, 9 December 2021, https://www.ncbi.nlm.nih.gov/books/NBK539860/
[4] V. P. Dixit, N. K. Lohiya, M. Arya, and M. Agrawal, “The Effects of Chemical Occlusion of Vas Deferens on the Testicular Function of Dog: A Preliminary Study,” Acta Eur Fertil, December 1975, vol. 6(4): 348–53, https://pubmed.ncbi.nlm.nih.gov/1217450/.
[5] J. J. van Lieshout, W. Wieling, J. M. Karemaker, and D. L. Eckberg, “The Vasovagal Response,” Clinical Science 81, no. 5 (November 1991): 575–86, https://pubmed.ncbi.nlm.nih.gov/1661644/.
Related Content








HLI staff writers bring you stories from the mission field and the latest information on life and family issues. All HLI articles are true to Catholic teaching.