- Human Life International
-
https://www.hli.org
-
Marriage and True Love versus “Contraceptive Love”
Posted By
Fr. Shenan J. Boquet
On
In
Catholic Marriage Resources,Contraceptives and Abortifacients,Effects of Contraception,Reproductive Technology,Spirit & Life Blog,The Church on Contraception |
7 Comments
It is not uncommon to question why the Catholic Church is interested in contraception. Further, because the subject is rarely preached about or spoken of, it is often unclear what exactly the Church teaches and why.
Modern society idolizes what it perceives as freedom, especially regarding human sexuality. Some assert that “love is love.” Sex is seen primarily as a matter of “self-expression” or “self-fulfillment.” This means one can love whoever they want and however they wish. However, proponents of this view never define what “love” is, or acknowledge the potential harm this view creates. After all, not everything someone does in the name of “love” is truly loving or beneficial to others. In other words, there is no understanding that genuine love involves an unwavering commitment of the will to seek the true good of the other, respecting their dignity and one’s own.
If one believes that “love is love,” any act is permissible, even when it violates the good that is relative to one’s sexual powers. The responsibility, morality, and dignity which belong to any Christian view of human sexuality are absent. This point of view inevitably leads to the “contraceptive mentality.” This is the mentality that one can have sex without consequences, but it must be free from the “burden” of conception. The result of encouraging this kind of sex leads to the destruction of any sound idea of marriage and family life. Human sexuality becomes unhinged from the necessity of self-denial. Sexuality is thus divorced not only from possible procreation but also from marriage itself. Once it is accepted that human sexuality is concerned primarily with “self-expression” or “self-fulfillment” there logically is no need to be married. Contraception is what makes this plausible.
Fr. Boquet on an NFP training mission
In rejecting contraception, the Church makes it clear that the choice to contracept has an intrinsic meaning. Procreation is an end of the marital act. To act against the nature of this end in contraceptive sex is to reject the order of the good that is inscribed in the nature of the conjugal act. In other words, a couple cannot reasonably define the act purely in terms of the end they have in view: the good end of enjoying sexual intercourse without risking conception because they believe that other responsibilities or circumstances would make it irresponsible for them to conceive. The means by which they achieve this end is contraception, which is always immoral. Its “wrongness” is that it is a contra-life choice.
Far from a never-ending list of “no’s,” Catholic teaching about contraception and marriage is primarily an affirmation of great goods to which the Church proclaims a resounding “Yes.” Her teaching is made “in the light of an integral vision of man and of his vocation, not only his natural and earthly, but also his supernatural and eternal vocation” (Humanae vitae[1], no. 7).
Because we are addressing human behavior and the values (goods) like marriage, conjugal love, and procreation that people pursue, the Church is concerned that these be valued in themselves and not be compromised. Furthermore, the Church not only has a vested interest in the good of Her sons and daughters but also in “the well-being of the individual person and of both human and Christian society [which] is closely bound up with the healthy state of conjugal and family life” (Catechism of the Catholic Church[2], no. 1603).
The Good of Conjugal Life
Marriage is a life-long covenantal relationship between one man and one woman. In this exclusive and indissoluble union, spouses enrich one another’s lives, so that their mutual love might give rise to new life. Despite the many variations marriage has undergone through the centuries, it is “not a purely human institution,” teaches the Catholic Church[2].It is not a creation of man, but an institution of nature that has been divinely ordained by God: “The vocation to marriage is written in the very nature of man and woman as they came from the hand of the Creator” (Catechism, no. 1603). Marriage is “the wise institution of the Creator to realize in mankind His design of love” and the marriage between the baptized has been raised by Christ to the dignity of a sacrament (Humanae vitae[1], no. 8).
Love is by nature opposed to the rejection of another’s good, as well as one’s own good. Our bodies are not something we simply have. They are part of what we are. We are bodied persons, male or female. Additionally, sexuality is not something we have, but, like my body, it is something I am, hence, it is part of my body. And because fertility is an integral element of sexuality, which gives one the capacity of begetting human life through a bodily action, sexual intercourse is also a good to be valued. In other words, a couple who engages in sexual activity that thwarts the procreative end of sex is violating their own good and the good of the other. This includes the biological good, i.e., fertility and procreation.
Today, there are many attempts to redefine marriage, human sexuality, and how children are begotten. In Casti Connubii[3], Pope Pius XI speaks about the freedom of man and woman to enter into marriage. They choose to marry, which is an act of the will. However, this freedom doesn’t imply that they can change or ignore the nature of marriage or redefine it. The Holy Father says,
Though each individual marriage arises only from the free consent of each of the spouses, this freedom, however, regards only the question whether the contracting parties really wish to enter upon matrimony or to marry this particular person; but the nature of matrimony is entirely independent of the free will of man, so that if one has once contracted matrimony he is thereby subject to its divinely made laws and its essential properties (no. 6).
The 8 couples who had cohabitated were helped by HLI Nigeria to embrace chastity and get married.
Pope St. Paul VI, in Humanae vitae, describes the “essential properties” of marriage, saying “this love is above all fully human…it is a love which is total…is also faithful and exclusive…[and] this love is fecund” (no. 9). In other words, being human, the couples’ bodies are essential and what they do with their bodies is relevant. As a permanent union, spouses seek the good of the other in the context of total and mutual self-giving (exclusive). And united in one flesh, every act of conjugal love must be open to the gift of life (fruitful). This conveys a profound union between spouses through their total self-giving and receiving, and the conceiving of a child.
Because the inseparability of the unitive and procreative ends of marriage are essential elements, they cannot be separated from each other. This means that authentic sexual love involves willing what is good for oneself and for one’s spouse. Acts that reject the order of a human good, as in contraceptive sex, are contrary to the authentic love that is always to be expressed in the martial act.
Pope St. John Paul II summarizes it best when saying,
When couples, by means of recourse to contraception, separate these two meanings that God the Creator has inscribed in the being of man and woman and in the dynamism of their sexual communion, they act as “arbiters” of the divine plan and they “manipulate” and degrade human sexuality-and with it themselves and their married partner-by altering its value of “total” self-giving. Thus, the innate language that expresses the total reciprocal self-giving of husband and wife is overlaid, through contraception, by an objectively contradictory language, namely, that of not giving oneself totally to the other. This leads not only to a positive refusal to be open to life but also to a falsification of the inner truth of conjugal love, which is called upon to give itself in personal totality Familiaris consortio[4], no. 32).
Contraceptive sex expresses contempt for the human good of fertility in authentic spousal love, viewing it as an obstacle to be removed. Furthermore, we must consider the relation of the couple to the child when contraception fails. If a child is begotten, surely there will be some feeling of regret because the reason they chose contraception was to prevent a conception (contra-life). The means they chose failed them, which can lead them to consider abortion. Or, even if they choose life for their child, there may still be some residual feeling of disappointment. This perfectly captures the “contraceptive mentality.”
The Contraceptive Mindset
In societies across the globe, contraception and its “mentality” have become normative, simply a part of life and conjugal relationships. Contraception is the direct intention of preventing by mechanical or chemical means the possible natural and procreative consequence of sexual intercourse – conception. The purpose, therefore, is to separate intercourse from procreation so that the contracepting partners can enjoy the pleasures of sex without fear that their sexual activity will lead to the begetting of another human being.
Acceptance of contraception and its “mentality” is not confined to a segment of society. Scandalously, recent national studies reveal[5] that over 90% of Catholics in the United States report using some type of artificial contraception to limit or prevent childbearing. This is a crisis of catechesis within the Church. We are not doing enough to address the issue and form the faithful. We need teaching that requires a response from the Church’s pastors, from those preparing couples for marriage, catechists working with Catholic youth, and from Catholic schools and universities that are teaching Catholic sexual ethics.
A “mentality” is established when a person (or society) reacts automatically to a situation without thinking of the long-range consequences. It describes a pervasive mindset that is aware of the immediate benefit but fails to consider the future repercussions. This “mentality” is very difficult to correct because it is shielded by unconscious assumptions and preserved by consistent behavior and habit, making it very difficult to resist. For example, let us consider promiscuity. A person engages in promiscuous behavior because they seek pleasure, companionship, and gratification; however, there is little to no consideration of the consequences of such behavior – disease, emotional harm, or pregnancy.
The “contraceptive mentality” exists when sexual intercourse is separated from procreation, the mentality is assumed as normative, and in employing contraception, the couple severs themselves from all responsibility for a conception that might take place from contraceptive failure. It implies that a couple not only have the means to separate intercourse from procreation, but also the right or responsibility to do so. It is also important to remember that at the very core of the “contraceptive mentality” is a fear of something which is perfectly natural – a child.
Because of successful propaganda and the rejection of Judeo-Christian values concerning marriage, human sexuality, and family life, many people in our society, including Catholics, have the attitude that new human life is sometimes inconvenient and an unnecessary burden, rather than a sacred gift from God. This is what Pope St. John Paul II saw as a root cause of abortion, and he condemned it. When we see any human life as a troublesome burden we must manage, rather than a sacred gift entrusted to our care, there is a dangerous temptation to get rid of the “burden” by any means necessary.
HLI’s donors helped Yvette support herself and little Leila! Yvette was able to get a sewing machine and learn how to sew to create a small business.
As Father Paul Marx, Human Life International’s founder, predicted,
The foolproof contraceptive does not exist and sociological studies have shown, almost without exception, that intensive contraceptive programs, by emphasizing the prevention of unwanted pregnancies, also reinforce an intention not to bear an unwanted child under any circumstances; that is, there is a greater likelihood that women experiencing contraceptive failures will resort to abortion.
We should also recall the prophetic words of Pope St. Paul VI in Humanae vitae, who spoke of the consequences of the “contraceptive mentality,” warning specifically men about the consequences of their actions saying,
Let them first consider how easily this course of action could open wide the way for marital infidelity and a general lowering of moral standards…especially the young, who are so exposed to temptation – need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law.
Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection (no. 17).
Lest We Forget
The heroic efforts of pro-life, pro-family groups striving to end the violence of abortion must continue, but I propose that our efforts will never reach the intended result without also addressing the “contraceptive mentality.” Though the “contraceptive mentality” is the root from which abortion flows, it too is a symptom of something much deeper. The desired goal of the revolutionary architects of the “sexual revolution” was to unmoor human persons from their inalienable dignity and enslave them to their passions and base appetites. Sadly, this methodology has been tremendously successful – attitudes and behaviors have been greatly corrupted.
Exposing the violence of abortion is crucial, and we must continue to work toward removing this deep scar from our nation and world. However, many are afraid to address the fundamental issue that sustains the abortion industry – contraceptionand its mentality. If we truly want to put a permanent end to the violence of abortion and protect the sacredness of human life, marriage, and family life then we must confront this intrinsic evil that feeds the entire machine and reclaim the language that sustains an authentic understanding of life, marriage, and human sexuality.
UK Male Contraception Developing While Condom Manufacturers Eye India
Posted By
Marisa Cantu
On
In
Contraceptives and Abortifacients,Global Life and Family News |
No Comments
Condom manufacturers are eyeing India[6] as their next big consumer. Their twisted reasoning is that due to India’s population growth, though it has slowed in recent decades[7], the country has surpassed China in population[8] and become the most populous country on Earth. So, of course, greedy businessmen see this as an opportunity to sell their contraceptives under the guise of “better health.” India’s condom usage rates are low (as few as 5% of men in India use condoms). They are hoping that India will use their products to decrease their population. What a tragic view of the world! To see a large population not only as something to squash but also as something to benefit financially from is another result of the prominence of the culture of death – and a call to pro-lifers to continue in the good fight.
HLI marriage enrichment program in India
Elsewhere in the world, in the UK, 16 British men will be the first to try a hormone-free male contraceptive, YCT-529[9], in the initial test phase. This contraceptive, manufactured by YourChoice Therapeutics, suppresses Vitamin A, which in turn suppresses sperm production. YourChoice Therapeutics claims that YCT-529 is more effective than condoms and that the infertility that comes as a result of suppressing Vitamin A was “100% reversible, with no side effects” in pre-clinical studies.
We know that female birth control not only harms a couple spiritually, but also has devastating effects on health[10] and the environment[11]. This male contraceptive is still in its early stages, and it is unclear whether it will have adverse effects on male fertility and health.
All forms of contraception, interrupt the conjugal act and frustrates one of the ends of the act. The conjugal act has two ends – procreative and unitive. The gift of human sexuality was given to us by God for these two ends, and, by nature, was meant to be open to life. When we separate one of these ends from the conjugal act, the act itself becomes disordered and we begin violating our marriage vows, which included the promise to be open to life. We also begin to use our spouse as an object of pleasure rather than giving ourselves freely, openly, and selflessly to the other and receiving our spouse in a loving manner.
We shouldn’t accept such evils for our brothers and sisters around the world. Please pray for the success of HLI’s mission, that we are able to bring the gospel of life to the world and heal all those affected by contraception’s horrible effects.
Abortifacient Brief: Why Was Depo Provera Banned?
Posted By
Brian Clowes, PhD and Marisa Cantu
On
In
Contraceptives and Abortifacients |
8 Comments
The birth control shot, Depo-Provera (DP), is an injectable contraceptive drug that sometimes has an abortifacient effect. While the intention behind using it is simply to prevent pregnancy, it also possesses a long list of shocking risks and side effects.
IN a 1967 11-year trial, DP was tested on a disproportionate number of poor, black, and rural women without informed consent and without giving the women information on the drug’s serious side effects. Upjohn Pharmaceuticals performed this study in an incredibly sloppy manner. They ignored the annual reports required by the Food and Drug Administration, lost 93% of patient records so that no follow-up studies could be done, and neglected to report deaths and very serious side effects cause by DP.1
This meant that the data from the study was entirely meaningless and unusable. Not surprisingly, the FDA withheld approval of DP both at the beginning and at the end of the study, not only because of the way the study was conducted, but because of a proven elevation in the risk of breast cancer among its users. In 1983, the FDA refused approval of DP a third time.
But in 1992, the FDA approved it for use in the United States over the objections of pro-life groups and even several pro-abortion women’s organizations, including the National Women’s Health Network and the National Black Women’s Health Project. Those following the proceedings were convinced that the FDA caved in under intense lobbying by Upjohn and pressure brought by population control groups.2 In June of the following year, Canada’s Department of Health and Welfare prohibited the use of DP, saying that the drug did not meet Canadian safety standards as a method of birth control.3
Pfizer now owns the drug. Pfizer also manufactures Depo-subQ Provera 104, a subcutaneous injection of DMPA using a smaller needle. This dose is promoted as Sayana Press, which is heavily promoted primarily in African nations by Pfizer, the Gates Foundation and the Children’s Investment Fund Foundation.4
Even worse, the WHO has launched ECHO, a large clinical study conducted in 12 African sites to determine whether DP increases the risk of HIV. Why do these organizations insist on making third-world nations test subjects?
DP is now available in more than 90 countries and is particularly popular among population controllers in Africa and the Caribbean and among those “caring” for native peoples in Thailand and New Zealand. As with all other abortifacients that may pose a danger to Western women, DP was first extensively tested on Third World women. The World Health Organization (WHO) used DP on more than 11,000 women in Kenya, Mexico, and Thailand before it was submitted to the FDA for approval.5
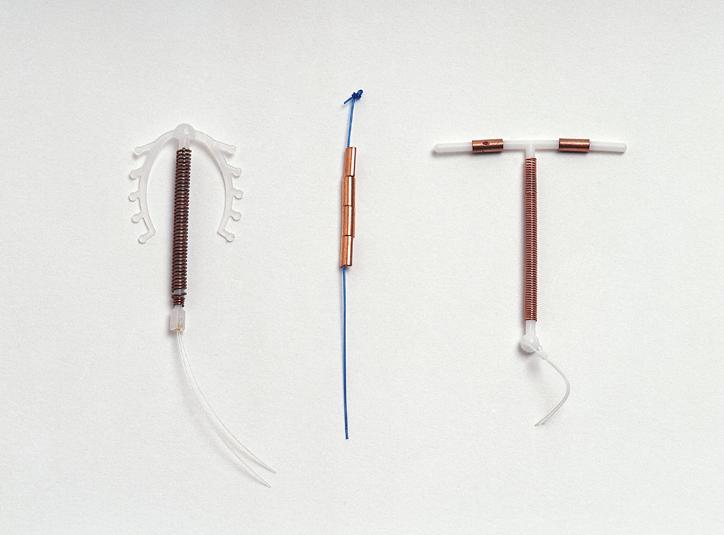
DP is one of a class of steroids that employ powerful hormones to control the female reproductive system. Other steroids in this class include birth control pills, the morning-after pill (MAP) and emergency contraception (EC), the implantables (Norplant, Jadelle, and Implanon), and some of the intra-uterine devices (IUDs).
Photo by Hyttalo Souza
DP’s active ingredient is depot-medroxyprogesterone acetate (DMPA), a synthetic form of the natural hormone progesterone, originally developed for the treatment of uterine cancer in the 1950s. Women receive 150 milligrams of DMPA via deep intramuscular injection every three months.
DP has three modes of action, similar to other methods of birth control that employ artificial progesterones as active ingredients:
It prevents ovulation (the release of an egg from the ovary).
It inhibits the entry of sperm through the cervix by altering the cervical mucus.
It alters the lining of the uterus such that, should a fertilized egg reach the uterus, it would have difficulty implanting.6
According to Upjohn’s patient information pamphlet on DP, the compound “inhibits the secretion of gonadotropins which, in turn, prevents follicular maturation and ovulation and results in endometrial thinning.”7
In other words, Upjohn acknowledges that Dep-Provera sometimes acts as an abortifacient[16].
The authoritative Contraceptive Technology confirms that DP causes early abortions. It alters the endometrium (the lining of the uterus) so that its degree of receptivity to the blastocyst (very early developing human being) is significantly decreased. According to Contraceptive Technology, “Other contraceptive actions include the development of a shallow and atrophic [thinning] endometrium.”8 When DP works in this way, it is an abortifacient.
Many women’s menstrual cycles continue when using DP, 43% after 12 months and 32% after 24 months.9 This data shows that the compound does not completely suppress ovulation in a large percentage of women who use this drug, so many early abortions occur.
Cemetery where crosses mark loss of the Unborn. Image: courtesy of LifeSiteNews.
Adverse Reactions to Depo-Provera
Current patient information pamphlets on DP list more than sixty adverse reactions suffered by women who use the compound, including these:
Women on DP report an average weight gain of 5.4 pounds in the first year and 16.5 pounds over six years.
Many users also experience osteoporosis (loss of bone mass) and a higher incidence of broken bones.10 The onset of osteoporosis is cumulative (Gets worse the longer a woman is on DP), remains long after the injections have ceased, and in many cases is irreversible. Because of this danger, the FDA ordered Pfizer to put a black box warning (its strongest warning) on its patient information pamphlets.11
In women who have used DP for the first time within the last four years, and who are under 35 years of age, the risk of breast cancer increases 129%.12 Use of DP may be associated with ectopic pregnancy, thrombophlebitis (inflammation of blood vessels associated with blood clots), pulmonary embolism (obstruction of the pulmonary artery by a blood clot, air bubble, or other material), cerebrovascular disorders, and partial or complete loss of vision in mothers, and polysyndactyly (webbing and extra digits of the hands and feet) hypospadias (genital tract abnormalities) and chromosomal anomalies among infants born to them.
More than 5% of users suffer headaches, nervousness, abdominal pain or discomfort, dizziness, or asthenia (weakness or fatigue).
Between 1 and 5% report one or more of the following ailments: decreased sexual desire or anorgasmia, depression, nausea, insomnia, abnormal vaginal discharges, pelvic and breast pain, rashes, hot flashes, swelling, vaginitis, and acne.
A study by the Gates Foundation in 2011 found that DP was likely to more than double[15] HIV rates among African women.
Other serious side effects include chest pains, pulmonary embolisms, allergic reactions, anemia, racing heart rate, abnormal blood chemistry, rectal bleeding, breast lumps or nipple bleeding, paralysis, facial palsy, abnormal growth of the uterus, varicose veins, and deep vein thrombosis.
Women who use Depo-Provera Contraceptive Injection (Depo-Provera CI) may lose significant bone mineral density. Bone loss is greater with increasing duration of use and may not be completely reversible [see Warnings and Precautions (5.1)].
It is unknown if use of Depo-Provera CI during adolescence or early adulthood, a critical period of bone accretion, will reduce peak bone mass and increase the risk for osteoporotic fracture in later life [see Warnings and Precautions (5.1)].
Depo-Provera CI is not recommended as a long-term (i.e., longer than 2 years) birth control method unless other options are considered inadequate [see Indications and Usage (1) and Warnings and Precautions (5.1)].
Further, DP was banned in 1978 in the US[20] for contraceptive uses over concerns about the carcinogen effects, despite the WHO and the International Planned Parenthood Fund endorsing its use in third-world nations. It has also been used to castrate criminals[21]. Additionally, many women do not know that DP should only be used for a maximum of two years under normal circumstances. Thus, some take DP for many years beyond and suffer the side effects.
A woman who is suffering from the side effects of this drug has no way to rid herself of the pernicious chemical except by waiting several months.
Abuses of the Birth Control Shot
From the point of view of a population controller, DP is very desirable because it can be controlled by medical professionals. It also causes three or more months of sterility and requires less operator skill to implement than sterilization, implantation of Norplant, or insertion of an IUD.
When my wife Kathy and I were in Uganda…we frequently saw white “Reproductive Health Unit” pickup trucks zooming through the countryside. These RHUs usually consist of two or three young men with little or no medical training who are given a few hours of instruction, a box of Depo shots and other types of birth control, and orders to go out into the country and get as many women as they can on birth control under a quota and reward system. We spoke with several groups of women who were victimized by these teams, some of whom said that they were injected with Depo after being told that it was an anti-malaria shot.
In January 2013, the Israeli health ministry discontinued a program targeting Ethiopian Jews in the country without informed consent.13
The white owners of commercial farms in Zimbabwe forced their black female workers to accept DP shots, and as a result, the drug was banned in 1981.14
In 2002, after widespread abuses, the Indian government ceased distribution of both Norplant and DP.15
Such efforts to target poor women have been ramped up significantly by Melinda Gates’ 2012 Family Planning Summit, with the cooperation of the International Planned Parenthood Federation (IPPF), the United States Agency for International Development (USAID), the United Nations and, of course, Pfizer, which stands to make billions of dollars of profit annually from the sale and distribution of the various types of DP. Indeed, they have recently expanded their partnership to continue distributing DP (now called Sayana® Press[23], which is simply a new form of DP) for cheap to specifically low-income nations.
Additionally, the UN has outlined “sustainable development goals” (SDGs) they hope to realize by 2030[24]. One of these is “…to ensure universal access to sexual and reproductive health-care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programmes.” No wonder businesses like the Gates Foundation, IPPF, or Pfizer are pushing so hard to deliver contraceptives to women in developing nations, as the UN fully supports this venture. It is curious why such large businesses insist on controlling the fertility of women in developing nations. The contents of the Kissinger Report[25] give us some clues.
Conclusion
Common ground between hard-core pro-abortion and pro-life groups is almost nonexistent. However, almost all of us agree that the birth control shot Depo-Provera poses an unacceptable health risk to women, especially those who are poor. We also agree that DP is being used to target both poor minority women in the United States and in developing nations.
It is time to speak the truth about Depo-Provera.
This article was originally published in April 2017 by Dr. Brian Clowes and was most recently updated in January 2024 by Marisa Cantu.
+ Endnotes
[1] Andy Smith. “Better Dead Than Pregnant: The Colonization of Native Women’s Reproductive Health,” in Jael Silliman and Anannya Bhattacharjee (editors). Policing the National Body: Race, Gender, & Criminalization [Cambridge, Massachusetts: South End Press], 2002.
[2] “Contraceptives: Case for Public Enquiry.” Economic and Political Weekly, Volume 29, Number 15 (April 9, 1994), pages 825–826.
[3] Gwen Duggan, Vice-President of Women for Women’s Health. “Depo-Provera and Women’s Health.” The Vancouver Sun, February 1993.
[4] Jane Dreaper. “The One Dollar Contraceptive Set to Make Family Planning Easier.” BBC News, November 15, 2014 at http://www.bbc.com/news/health-30026001.
[5] Karen Hawkins and Jeff Elliott. “Seeking Approval.” Albion Monitor, May 5, 1996.
[6] University of California at Berkeley University Health Services, Tang Center. “Depo-Provera for Contraception,” March 28, 2011. See also October 2010 patient information pamphlet by Physicians Total Care.
[7] Patient information brochure. “Now Available in the U.S.: Depo-Provera Contraceptive Injection.” Upjohn Pharmaceuticals, December 1992. The pamphlet also says that Depo-Provera “[has a] contraceptive effect produced by inhibiting the secretion of gonadotropins (FSH, LH), which prevents follicular maturation and ovulation.… Suppresses the endometrium [the mucous membrane lining the uterus] and changes cervical mucus.”
[8] Robert A. Hatcher, et. al. Contraceptive Technology (18th Revised Edition) [New York City: Ardent Media, Inc.], 2004. Chapter 20, “Depo-Provera Injections, Implants, and Progestin-Only Pills (Minipills),” pages 461 to 494.
[9] Patient information brochure. “Now Available in the U.S.: Depo-Provera Contraceptive Injection.” Upjohn Pharmaceuticals, December 1992.
[10] On October 30, 1992, the Los Angeles Times, Houston Chronicle, and Minneapolis Star-Tribune, among other major newspapers, reported, “Use of Depo-Provera may be considered among the risk factors for developing osteoporosis. The rate of bone loss is greatest in the early years of use.” See also Health Canada’s Canadian Adverse Drug Reaction Monitoring Program (CADRMP), Marketed Health Products Directorate, “New Safety Information on the Use of DEPO-PROVERA (medroxyprogesterone acetate suspension for injection, 150 mg IM) associated with Bone Mineral Density Changes,” July 7, 2005.
[11] United States Food and Drug Administration. “Black Box Warning Added Concerning Long-Term Use of Depo-Provera Contraceptive Injection,” November 17, 2004.
[12] On October 30, 1992, the Los Angeles Times, Houston Chronicle, and Minneapolis Star-Tribune, among other major newspapers, reported, “A slight increased overall risk of breast cancer has been associated with use in women under 35 years of age whose first exposure to the Depo-Provera Contraceptive Injection was within the previous four years. Other complications include weight changes, menstrual irregularities, headache, dizziness, nervousness, abdominal pain or discomfort, and asthenia (weakness or fatigue).”
[13] “Israel Accused of Dooming Ethiopian Baby Boom.” RT, February 24, 2010; Renee Ghert-Zand. “Shocking Decline in Ethiopian Israeli Birthrate.” The Jewish Daily Forward, December 10, 2012; Talila Nesher). “Israel Admits Ethiopian Women were Given Birth Control Shots.” Haaretz, January 27, 2013.
[14] Amy Kaler (Department of Sociology, University of Minnesota). “A Threat to the Nation and a Threat to the Men: The Banning of Depo-Provera in Zimbabwe, 1981.” Journal of Southern African Studies (Volume 24, Number 2), pages 347 to 376.
[15] Andy Smith. “Better Dead Than Pregnant: The Colonization of Native Women’s Reproductive Health,” in Jael Silliman and Anannya Bhattacharjee (editors). Policing the National Body: Race, Gender, & Criminalization [Cambridge, Massachusetts: South End Press], 2002.
Birth Control: Is the Pill an Abortifacient?
Posted By
Brian Clowes, PhD and Marisa Cantu
On
In
Contraceptives and Abortifacients |
47 Comments
What exactly is “abortifacient” birth control, and is “the Pill” an abortifacient?
Contraceptives are methods of birth control that place a physical barrier between sperm and egg, such as condoms and diaphragms. By contrast, abortifacients are hormonal-based methods of birth control that often cause early abortions. In 2019, an estimated 27% of women were using such methods[26] in the United States alone.The principal method[27] of abortifacient birth control is “the Pill,” which first became widely used in the late 1960s and helped fuel the Sexual Revolution.
Let’s review what birth control does.
Is the Pill an Abortifacient?
“Contraceptive” means a method of birth control that prevents pregnancy by placing a physical barrier between them. However, all birth control pills and the other hormonal methods of birth control on the market today function as abortifacients part of the time. The Pill often ends early pregnancies by preventing implantation of an already fertilized egg, or very early human being.
Human development from fertilization to birth
Over the past half-century, three general classes of birth control drugs have been manufactured in the United States and other countries — the high-dose pill, the combination pill and the progestin-only “minipill.”
The old high-dosage drugs were rarely abortifacient in their modes of action. They mostly worked by thickening cervical mucus and inhibiting ovulation. Sometimes, however, breakthrough ovulation occurred, and so the older drugs were occasionally abortifacient in their actions.
Eventually the older “high-dose” drugs gave way to the new “low-dose” drugs. Ortho/Johnson & Johnson, G.D. Searle/Monsanto, and Syntex, the three largest manufacturers of abortifacient birth controls in the United States, voluntarily withdrew their “high-dose” products from the U.S. market in 1988 on the advice of the U.S. Food and Drug Administration (FDA). These were among the last commercially-available pills in the United States containing more than 50 micrograms of estrogen.1
Each of the newer low-dose pills has between 50 and 3,000 micrograms of a variety of compounds containing progestin and between 10 and 50 micrograms of artificial estrogen in the form of ethinyl estradiol or mestranol. This is a tremendous drop in estrogenic potency compared to the high-dose drugs.2
The newer low-dosage combination and progestin-only pills have three modes of action:3
The first of the three modes of action is the suppression of ovulation. When a woman ingests birth control drugs, they hijack her reproductive system. Her body is hormonally “tricked” into acting as if it is continuously pregnant. During those months that ovulation is suppressed, the mode of action is contraceptive (not abortifacient) in nature.
The second mode of action is also contraceptive in nature. The drugs cause changes in the consistency and acidity of cervical mucus, making it more difficult for sperm to penetrate and live in the cervix.
The third mode of action is abortifacient. The pills cause changes in the endometrium (lining of the uterus), making implantation more difficult. It transforms the endometrium from a welcoming, lush forest into a barren, sterile desert. In a cycle where ovulation was not prevented and fertilization takes place, it causes a “silent abortion.”
Indeed, even the Guttmacher Institute (the former research arm of Planned Parenthood) admitted that contraceptives can prevent implantation of a fertilized egg[28]. Conveniently, they claim that pregnancy only occurs once implantation begins, instead of when a unique DNA code and living creature is created at fertilization. But this doesn’t make sense. Why would pregnancy only begin once the newly created child arrives in a specific place (e.g., in the uterus versus the ovary), rather than when the child is actually created?
Birth Control Today
There are now more than 200 brands and varieties of progestin/estrogen pills on the market. All of them — from Alesse to Zovia — sometimes prevent implantation of the developing human being. The low-dose pill works in essentially the same manner as the old high-dose pill. However, a much higher percentage of ovulation occurs in women who use the low-dose drugs due to their lower estrogen dose. This means that all of the newer oral “contraceptive” drugs act as abortifacients at least part of the time.4
Thus, women who use these drugs frequently conceive. In order to prevent the continuation of pregnancies in these cases, the low-dose drugs also prevent implantation, thereby acting as back-up abortifacients.
Several studies have shown that women on the low-dose pills experience an early “silent abortion” during a wide range of 2% to 65% of their cycles, depending upon the formulation used.5
The mechanisms of action of minipills (progestin-only pills, or POPs) are similar to that of the standard progestin/estrogen combination.6
These progestin-only pills interfere with implantation by affecting the endometrium, thickening the cervical mucus, and suppressing ovulation in some women by reducing the presence of follicle-stimulating hormone (FSH).
The manufacturers of the minipills acknowledge this mode of action. For example, Syntex Laboratories announced that its progestin-only drug Norinyl “did not interfere with ovulation….It seems to affect the endometrium so that a fertilized egg cannot be implanted.”7
The Searle Pharmaceutical Corporation developed Enovid, the first birth control pill, in the late 1950s.
Enovid and other high-dose birth controls have generally fallen out of favor in the United States. However, they are still used in some developing countries. They contain from 1000 to 12,000 micrograms of progestin and/or 60 to 120 micrograms of estrogen, a natural female hormone. This high dosage had a variety of side effects, including blurred vision, nausea, weight gain, breast pain, cramping, irregular menstrual bleeding, headaches, and possibly breast cancer.
Beginning in about 1975, drug makers, reacting to extensive publicity about the severe side effects of the high-dosage drugs, steadily decreased the content of estrogen and progestin in their products.
However, the patient information pamphlets continue to feature a long list of very serious side effects. A review of some of the most common brands shows many similar effects.
These include blood clots, venous thromboembolism (VTE), stroke, hyperkalemia (high potassium levels), carcinomas of the breasts and reproductive organs, liver disease, high blood pressure, numbness, chest pain, cerebral thrombosis, and gallbladder disease. They also list a host of less dangerous side effects, to include headaches and nausea, weight gain, back pain, skin pigmentation changes, bleeding irregularities, depression and breast tenderness, most of which have an incidence of between 8% and 33%.8
“Progressives” frequently virtue signal by bragging about their “responsible and non-exploitative” methods of consumption. But they have no problem at all with the horrible way that poor women in other nations have been treated by the big pharmaceutical corporations when testing their birth control products.
In keeping with its defensive anti-lawsuit strategy, Searle tested its Enovid birth control on poor Puerto Rican women before concluding in 1961 that it was safe for women in North America and Europe to use.9
Experimentation on foreign women has been a typical tactic of the leading pharmaceutical corporations. They have often tested abortifacient chemicals and devices on poor women in developing countries to make any mistakes or serious health problems easier to cover up. Women in these nations had little recourse when their health[30] was destroyed or damaged by this kind of testing, because the investments of large pharmaceutical companies bring huge amounts of money to their homelands. Thus, any protest against the testing programs can easily be suppressed by corrupt local or national governments. We do not know if such testing on poor women in developing nations is still being conducted. But the plans laid out in the now declassified Kissinger Report[31] describe secretive ways to continue such operations while trying to conceal them.
Why don’t we know whether such heinous practices are currently happening? This may be due to worldwide condemnation of such practices in the past, causing a greater degree of secrecy, or simply a move to all-animal testing.
One of the most dangerous population suppression organizations on earth, the Population Council, produced the insertable abortifacient Norplant. The Population Council was funded in this effort by the United States Agency for International Development (USAID), and tested Norplant on poor women in several Asian nations. Doctors testing the drug refused to remove it from Bangladeshi women who were suffering horribly from its disastrous side effects. Korean women were not informed that Norplant was experimental and were not told of any side effects. Many women were bribed to use the drug and instructed not to report side effects so that the test program results would be skewed to show lower rates of health problems. When women became too sick to avoid seeking medical attention, proper care was withheld from them.10
The American College for Obstetrics and Gynecology reports the prevalence of ectopic pregnancies[34] based on method. The results were from a survey of 9,256 women. For those using no contraceptive or condom, about 1.37% of pregnancies surveyed were ectopic. For users of levonorgestrel intra-uterine devices (IUDs), the incidence rose to 7.84%. Cooper IUDs had lower rates, at 4.17%. Implant users and depot medroxyprogesterone acetate users were reported as having 0 ectopic pregnancies in the survey. Finally, users of oral contraceptives, a contraceptive patch, or vaginal ring reported 0.28%.
Other sources report varying numbers. The Australian government’s Better Health Channel says the prevalence of ectopic pregnancy[35] is about 5% in women using copper IUDs or minipills, 10% in women using implants, and up to 50% for users of hormone-releasing IUDs.
The copper IUD is an abortifacient.
While it’s important to acknowledge that not every pregnancy that occurs despite contraception will be ectopic, it is worthwhile to consider the effects the pill has[36] on a woman’s body. Thus, if you are pregnant, it is essential to get an ultrasound to locate where the child implanted.
If You Take Birth Control While Pregnant, Will It Kill the Baby?
If you’re pregnant while taking birth control, what are the effects? Studies on this topic are inconclusive. Some studies show that taking birth control after implantation carries no risk to the pregnancy, and others say it may carry a risk of birth defects. The reason there is so little data on this topic is due to the unethical nature of having pregnant women take birth control to study whether it contributes to birth defects or a miscarriage. That being said, if you are taking birth control, it is better to stop taking it when you are pregnant.
Another form of birth control is the aforementioned IUD. As with any form of birth control, IUDs are not 100% effective at preventing pregnancy. Pregnancies with IUDs[38] carry an increased risk of late miscarriage, premature birth, and bleeding, among a few other risks.
What Now?
What is one to do if one wants to get off birth control, but is afraid? Don’t be. You can stop taking birth control fairly easily and quickly. If you are using the patch, pills, or the ring, you are able to stop completely at any time. If you’re using a hormonal implant or IUD, you must schedule an appointment with your doctor to have these removed. Trying to remove them yourself can result in serious harm or complications. If you’re using shots like Depo-Provera, simply do not receive the next shot.11
Women coming off birth control[39] sometimes experience cramping, irregular periods, or acne, among other effects. Fertility will return in most cases. That’s a good sign of health.
Summary
Although it is routinely referred to as the “oral contraceptive pill” or OCP, the Pill is not conception control, or contraception. Though that may have been the original intention, developments in medicine have led to the creation of drugs and other devices that also act as abortifacients in cases where conception is not prevented. Some of these have truly Orwellian names such as the IUCD, the “Intrauterine Contraceptive Device,” and the UTS, or “Uterine Therapeutic System.”12
In other words, oral “contraceptives” are not true contraceptives.
This article was originally published in April 2021 by Dr. Brian Clowes and was most recently updated in October 2023 by Marisa Cantu.
+ Endnotes
[1] Bogomir M. Kuhar, Ph.D. “Pharmaceutical Companies: The New Abortionists.” Reprint 16 from Human Life International, 4 Family Life Lane, Front Royal, Virginia 22630.
[2] Review of about 150 pill compositions in patient information pamphlets downloaded from the National Institute for Health’s website DailyMed[40]. Birth control pills contain artificial progestins with many different formulations, including levenorgestrel, norethindrone, desogestrel, drospirenone, norgestrel, ethynodiol diacetate and gestodene.
[3] “Minipill (Progestin-Only Birth Control Pill).” Mayo Clinic, January 13, 2023. https://www.mayoclinic.org/tests-procedures/minipill/about/pac-20388306#:~:text=The+minipill+thickens+cervical+mucus,may+keep+you+from+ovulating; “Progestin-Only Hormonal Birth Control: Pill and Injection.” ACOG, January 2023. https://www.acog.org/womens-health/faqs/progestin-only-hormonal-birth-control-pill-and-injection#:~:text=How+do+progestin%2Donly+pills,does+not+do+so+consistently.
[4] Patient information pamphlets downloaded from the National Institute for Health’s website DailyMed[40].
[5] Walter L. Larimore, M.D. and Joseph B. Stanford, M.D., M.S.P.H. “Postfertilization Effects of Oral Contraceptives and Their Relationship to Informed Consent.” Archives of Family Medicine (American Medical Association), February 2000 (Volume 9). Interestingly, a postscript by Dr. Larimore describes how he and his wife stopped using the birth control pill and how he stopped prescribing it due to its abortifacient action. To see a complete book on the abortifacient action of the pill, which includes citations of many scientific studies on this topic, read Randy Alcorn’s Does the Birth Control Pill Cause Abortions?[41]
[6] “Minipill (Progestin-Only Birth Control Pill).” Mayo Clinic, January 13, 2023. https://www.mayoclinic.org/tests-procedures/minipill/about/pac-20388306#:~:text=The+minipill+thickens+cervical+mucus,from+implanting+in+the+womb.
[7] United Press International news release in the Cincinnati Post, January 11, 1973.
[8] “Azurette (28) Oral: Uses, Side Effects, Interactions, Pictures, Warnings & Dosing.” WebMD. Accessed October 19, 2023. https://www.webmd.com/drugs/2/drug-151684/azurette-28-oral/details#:~:text=Nausea%2C+vomiting%2C+headache%2C+bloating,first+few+months+of+use; Durbin, Kaci, ed. “Yaz: Side Effects, Dosage & Uses.” Drugs.com, 2023. https://www.drugs.com/yaz.html; “Heather Side Effects: Common, Severe, Long Term.” Drugs.com. Accessed October 19, 2023. https://www.drugs.com/sfx/heather-side-effects.html; Superdrug Online Doctors. “Microgynon Side Effects.” Superdrug Online Doctors. Accessed October 19, 2023. https://onlinedoctor.superdrug.com/microgynon-side-effects.html; “Yasmin Side Effects: Common, Severe, Long Term.” Drugs.com, May 4, 2023. https://www.drugs.com/sfx/yasmin-side-effects.html.
[9] Bogomir M. Kuhar, Ph.D. “Pharmaceutical Companies: The New Abortionists.” Reprint 16 from Human Life International, 4 Family Life Lane, Front Royal, Virginia 22630.
[10] UBINIG (Bangladesh) Research Report. “Norplant, the Five-Year Needle: An Investigation of the Norplant Trial in Bangladesh from the User’s Perspective.” Reproductive and Genetic Engineering: Journal of International Feminist Analysis, 1990 (Volume 3, Number 3); Elizabeth Sobo. “NORPLANT: Lab-Tested on Third World Women.” Our Sunday Visitor, February 3, 1991, pages 10 and 11.
[11] “Your Guide to Going off of Birth Control.” Cleveland Clinic, January 19, 2023. https://health.clevelandclinic.org/your-guide-to-going-off-of-birth-control/.
[12] E.B. Connell. “The Uterine Therapeutic System: A New Approach to Female Contraception.” Contemporary OB/GYN, June 1975, pages 49 to 55.
What Are Abortifacients?
Posted By
HLI Staff
On
In
Contraceptives and Abortifacients |
10 Comments
An abortifacient[42] “an agent (such as a drug) that induces abortion.” After an egg is fertilized, abortifacients kill the unborn child. However, manufactures often market these drugs under the name “contraception” to make them more appealing to consumers. Abortifacients are different from contraceptives in that they do not prevent an egg from being fertilized. Rather, they act after fertilization to kill a child in the earliest stages of development.
Many Contraceptives Are Really Abortifacients
In 1963, the United States Department of Health, Education and Welfare shared the widely held definition of abortion[43] as “all the measures which impair the viability of the zygote at any time between the instant of fertilization and the completion of labor.” Indeed, until the mid-1960s, scientists universally acknowledged that human life begins[16] at the moment of fertilization of the ovum by the sperm somewhere in the Fallopian tube.
In order to make abortion-causing methods more palatable in societies that still widely rejected abortion, and to circumvent laws designed to prohibit abortion, the promoters of birth control realized that they had to blur the line between conception-preventing (contraceptive) and early abortion-causing (abortifacient) actions. They did this by changing the definition of “conception” from fertilization (union of sperm and ovum) to implantation. Under the new definition of “conception,” if a device or drug―such as an IUD or hormonal contraception―prevents implantation, then no abortion takes place.
The “family planning” industry finally succeeded in 1965, when the American College of Obstetricians and Gynecologists published its first Terminology Bulletin, stating: “Conception is the implantation of a fertilized ovum.”1It is important to note that this change in terminology was clearly not based upon new scientific findings but was a political decision to appease birth control activists.
Dr. J. Richard Sosnowski, head of the Southern Association of Obstetricians and Gynecologists, a member group of ACOG, acknowledged this nonscientific change almost two decades later:
I do not deem it excellent to play semantic gymnastics in a profession…. It is equally troublesome to me that, with no scientific evidence to validate the change, the definition of conception as the successful spermatic penetration of an ovum was redefined as the implantation of a fertilized ovum. It appears to me that the only reason for this was the dilemma produced by the possibility that the intrauterine contraceptive device might cause abortion.2
In other words, manufacturers of abortifacients call their products “contraceptives” not because they prevent conception but because they prevent implantation. Such methods are sometimes called “contragestions[44],” referring to those abortive products that either prevent a fertilized egg from attaching to the uterus, or otherwise dissolving it or expulsing it from the uterus. This terminology does not tell the truth, and it does not change the reality – that these methods are killing an unborn child.
As we shall see, this game of words is unscientific.
What Is True Contraception?
A true contraceptive method prevents conception in one or more of these ways:
It places an actual mechanical barrier (such as a condom or cervical cap) between the sperm and ovum to prevent them from uniting.
It thickens the cervical mucus, preventing the easy travel of sperm.
It inhibits ovulation, preventing the release of a mature ovum.
It blocks the Fallopian tube or vas deferens through sexual sterilization.
When effective, each of these methods prevents a new human being from being created.
What Is an Abortifacient?
Recall that an abortifacient is “an agent that induces an abortion.” Depending on the type of abortifacient, the abortion happens by preventing the implantation of the early human being (blastocyst) in the uterus or by killing the preborn child shortly after implantation.
There are two distinct kinds of abortifacients. The first includes drugs and devices that continually maintain a certain level of hormones in the woman’s body, mimicking pregnancy. While these can also have a genuine contraceptive effect, each also has the potential to alter the lining of the uterus (endometrium) to prevent the implantation of a tiny human being.
“Emergency contraception”: These abortifacients have many forms and are sometimes called “morning-after pills[51].” They consist of high doses of the artificial steroids used in oral contraceptives. The most popular brand is Plan B.
The Input of Modern Science
Despite the birth control industry’s political victories in influencing the language of certain medical organizations, embryology (the field of science that specifically deals with the biological facts of the beginning of life) still holds that a new human being comes into existence at conception/fertilization.
Embryologists have found that from the first moment of creation, the new human being’s genetic code is complete, his sex is determined, and with proper nourishment in the womb he will continue to develop as every human being does. This is not a religious viewpoint; it is hard science.
There is also no scientific debate about the abortifacient effects of the drugs in question (though some drugs are still being tested), as preventing the tiny embryonic human being from implanting in the womb will certainly kill him. The manufacturers and promoters of these birth control methods, however, having largely won the debate over language, continue to market their products as “contraception.”
The patient inserts for all abortifacients are available online, and descriptions of how they operate to alter the endometrium are shown below. These products generally work to suppress ovulation and cause changes in the consistency of cervical mucus, making it more difficult for sperm to reach the ovum. These are true contraceptive effects.
However, as we have seen, these products also alter the uterine lining, making implantation much more difficult. In a cycle where ovulation was not prevented and fertilization takes place, a “silent abortion” will occur. Some examples of the way these “contraceptives” work are listed below:
Depo-Provera[15] “inhibits the secretion of gonadotropins which, in turn, prevents follicular maturation and ovulation and results in endometrial thinning.”
Nexplanon[52] uses hormones that “[stop] ovulation by preventing the release of an egg from the ovary; thins the lining of [the] uterus, which makes implantation of the egg more difficult; thickens mucus in the cervix, which makes it harder for the sperm to reach the egg.”
Intrauterine Devices (such as Mirena[53]): According to RX List, “Studies of Mirena and similar LNG IUS prototypes have suggested several mechanisms that prevent pregnancy: thickening of cervical mucus preventing passage of sperm into the uterus, inhibition of sperm capacitation or survival, and alteration of the endometrium.”
NuvaRing[54] contains “…2 types of female hormones – estrogen and progestin – which work together to prevent a pregnancy.” These two hormones prevent ovulation[55] by stopping the luteinizing hormone (LH) and the follicle-stimulating hormone (FSH) from being produced. LH and FSH are essential in ovulation. By blocking LH and FSH, estrogen and progestin prevent ovulation, meaning there is no egg released. If, however, an egg is released and fertilized, these hormones also alter[56] the uterine lining, thus making implantation difficult, if not impossible.
Plan B Contraception[57]: This “morning-after pill” works to prevent ovulation but can also prevent a baby from implanting in the uterus. According to the Polycarp Institute: “If both sperm and an egg are present and one does not see evidence of clinical pregnancy, then abortion is the most likely mechanism of action.”
Yasmin[58] “causes changes in [the] cervical mucus and uterine lining, making it harder for sperm to reach the uterus and harder for a fertilized egg to attach to the uterus.”
Abortifacients Harm the Mother
The patient information pamphlets for the above abortifacients reveal that, in addition to potentially causing an early abortion, they can harm the woman as well, as they can cause a variety of more than 80 side effects[45] depending upon the method.
Contraception was destroying Violet’s soul, and her health. Backed by HLI donors, missionary Veronica (right) helped her choose openness to life.
These side effects come from a powerful group of chemicals called steroids and synthetic progestogens and progestins. There’s a huge range of potential side effects – everything from paralysis, toxic shock syndrome, ectopic pregnancy, stroke, blood clots, [59]and heart attack[59], to the less serious hypertension, anemia, and varicose veins.
Some birth controls also increase the risk[60] of cervical and breast cancers.
You can read more about these side effects in our eight-page booklet that you can order from our store[62].
Risks of the Abortion Pill
Perhaps the most famous abortifacient is the abortion pill, also known as the mifepristone/misoprostol combination. Mifepristone works by blocking the hormone progesterone[49], which is necessary to continue a pregnancy. As a result, the newly formed baby is expelled from the uterus. This is often taken with misoprostol, which causes the uterus to contract and empty itself of the baby.
After the recent overturn of Roe v. Wade in 2022, the abortion pill has become increasingly difficult to acquire. More and more, women are being told they can take the pill at home – an incredibly dangerous suggestion.
If you or someone you know is struggling with an unplanned pregnancy, rest assured that help is available. There are people who care about you and want what’s best for you. Pregnancy resource centers[65] all across the nation offer help and support every day for women in crisis pregnancies.
This article was originally published in November 2021 and most recently updated in August 2023.
+ Endnotes
[1] American College of Obstetrics and Gynecology, Terminology Bulletin, “Terms Used in Reference to the Fetus,” Chicago: ACOG, September 1965.
[2] J. Richard Sosnowski, MD, “The Pursuit of Excellence: Have We Apprehended and Comprehended It?” American Journal of Obstetrics and Gynecology, September 15, 1984, page 117.
How Effective Are Condoms Against Pregnancy?
Posted By
HLI Staff
On
In
Contraceptives and Abortifacients |
7 Comments
The use of condoms is considered normal, almost compulsory, for many people engaging in sex today, whether married or unmarried. Of course, pro-lifers and Catholics oppose this unnatural device on the moral[66] level. It not only disrupts the mechanism of transmitting human life in the most direct way possible; it also encourages promiscuity with false promises of “preventing pregnancy” or diseases.
But even on the practical level, condoms don’t do what they are meant to! The condom “failure” rate (meaning the possible permission of natural pregnancy) is high, and the latex balloon carries with it a host of other practical problems.
(A note: this article uses scare quotes for phrases like “prevent pregnancy,” “failure,” and others, because these are talking points from the contraceptive worldview that divorce sex from procreation[12] as a natural end.)
How effective are condoms? How effective are they at “preventing pregnancy”? The answer to these questions: not very. In this article, we’ll cover the following points about the ineffectiveness of condoms:
Condom “failure” rate is high
Condoms do not “prevent pregnancy” over time
Condom promoters use irrelevant evidence
Condoms haven’t delivered statistically
Let’s begin.
1. Condom “Failure” Rate Is High
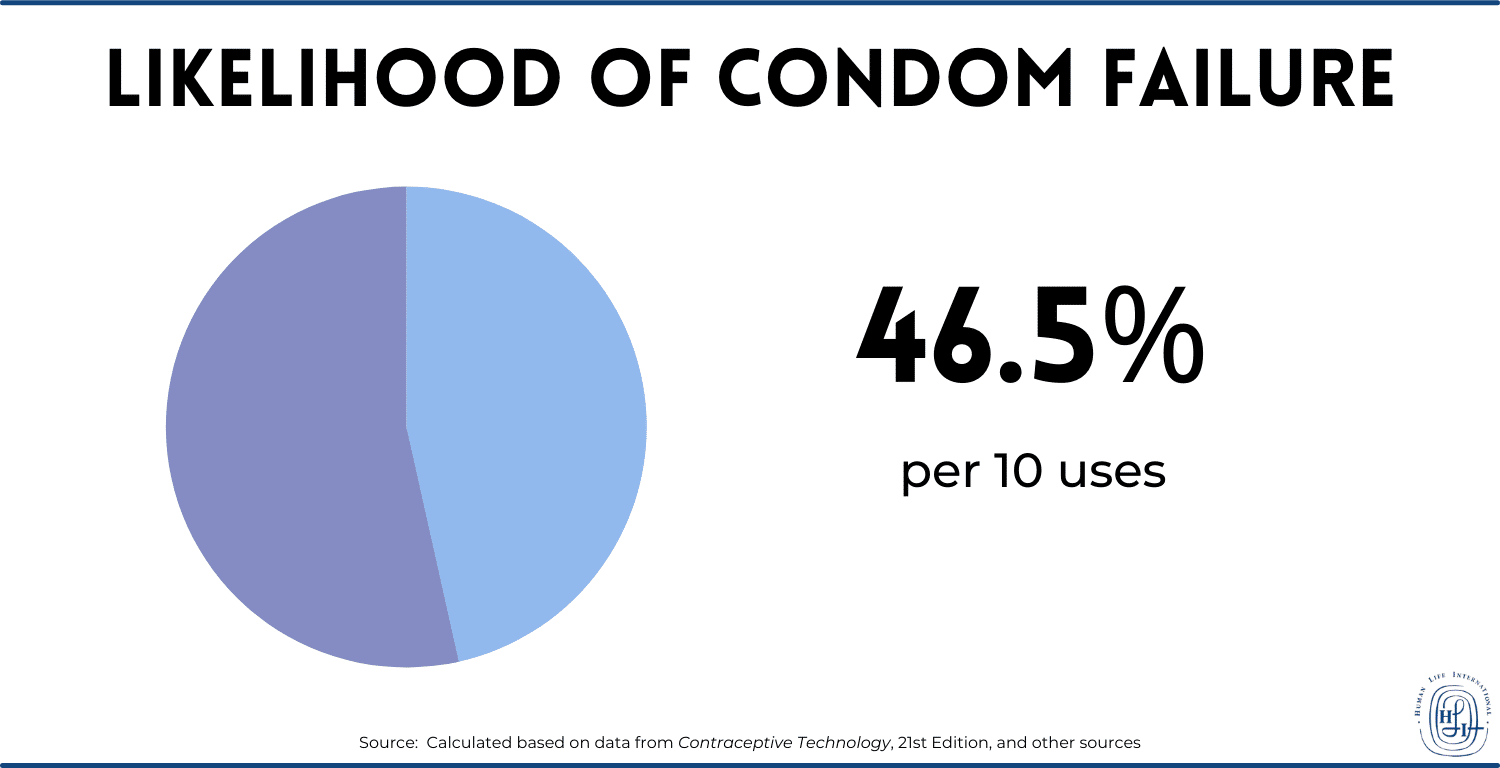
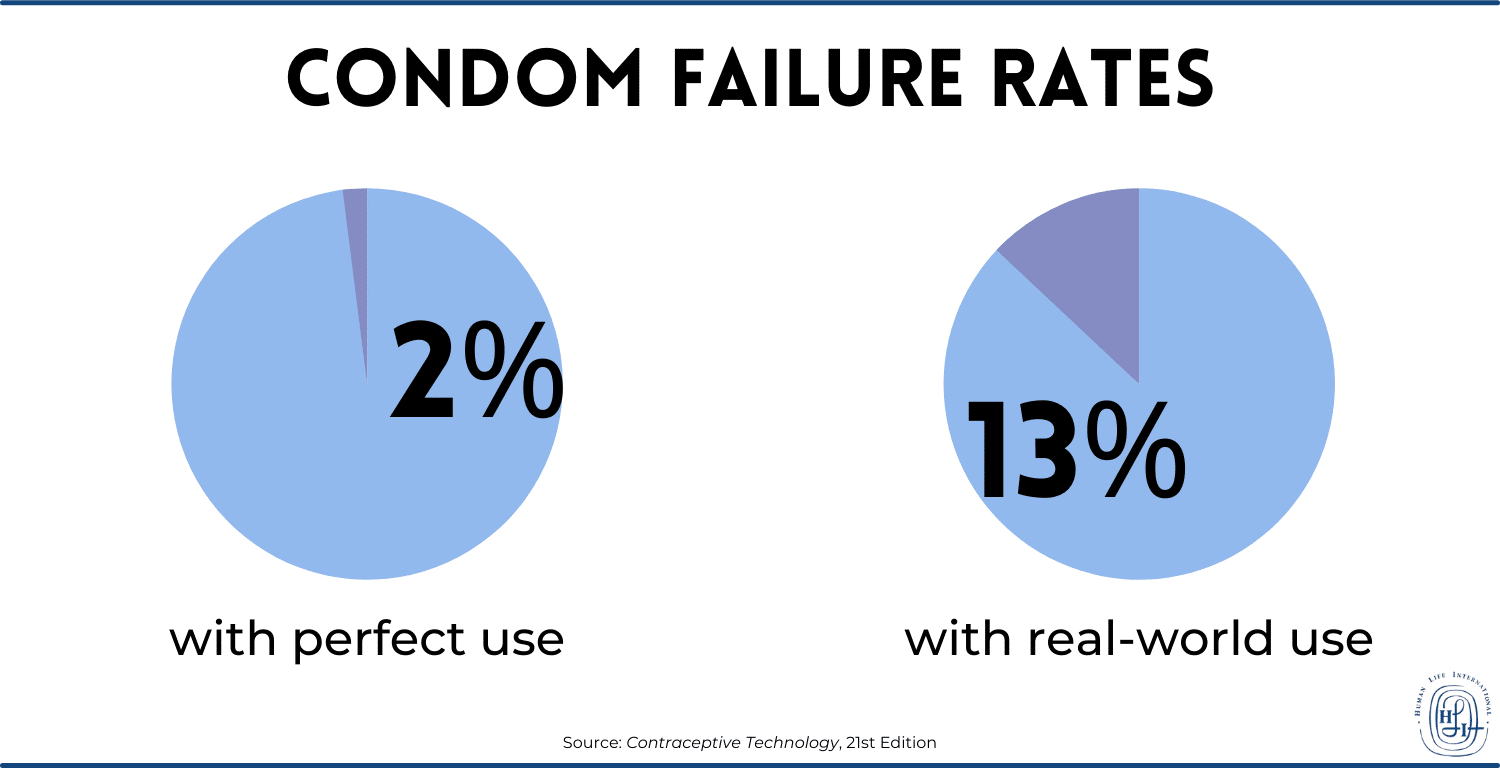
The male condom is the most commonly used barrier method of contraception in the world. But how effective are condoms? According to mainstream scientific sources, their efficacy has been grossly overstated by condom promoters. After the use of just 10, the probability of at least one “failure” is 46.51%, according to calculations done by Human Life International based on data from the authoritative Contraceptive Technology (21st Edition, 2018) and other sources[67].1
Twenty-three major studies of almost 60,000 condoms used during heterosexual intercourse in five different countries have found that 4% of all the condoms broke and 2.06% of them partially or completely slipped off, for a total “failure” rate of 6.06%. That means that about 1 in 17 uses results in condom “failure.” “Failure” means the possibility of pregnancy (in other words, the marital act may succeed in its natural end despite the interference of the condom). Even the highest-quality condoms used in the most “effective” manner possible by educated, monogamous, adult couples “fail” at a high rate under real-world conditions. This information is available from a Human Life International meta-analysis that draws on information in Contraceptive Technology (21st Edition, 2018) and other studies.2
Correct condom use is uncommon because it is complicated and involves significant attention to detail in moments when one is strongly distracted. A 2012 synthesis of 50 studies on condom use errors identified more than ten potential user errors, in addition to the issues of fit, slippage and breakage that are inherent to the condom itself.3 Several user errors were found to be extremely common, including failure to lubricate the condom (16.0%-25.8% of participants), incorrect withdrawal (43%-57% of condom use events), and incorrect storage (3.3%-19.1% of participants).4
These error rates are recorded from populations in the USA, Canada, and the British Isles, where education about correct condom use is widely accessible.
2. Condoms Do Not “Prevent Pregnancy” over Time
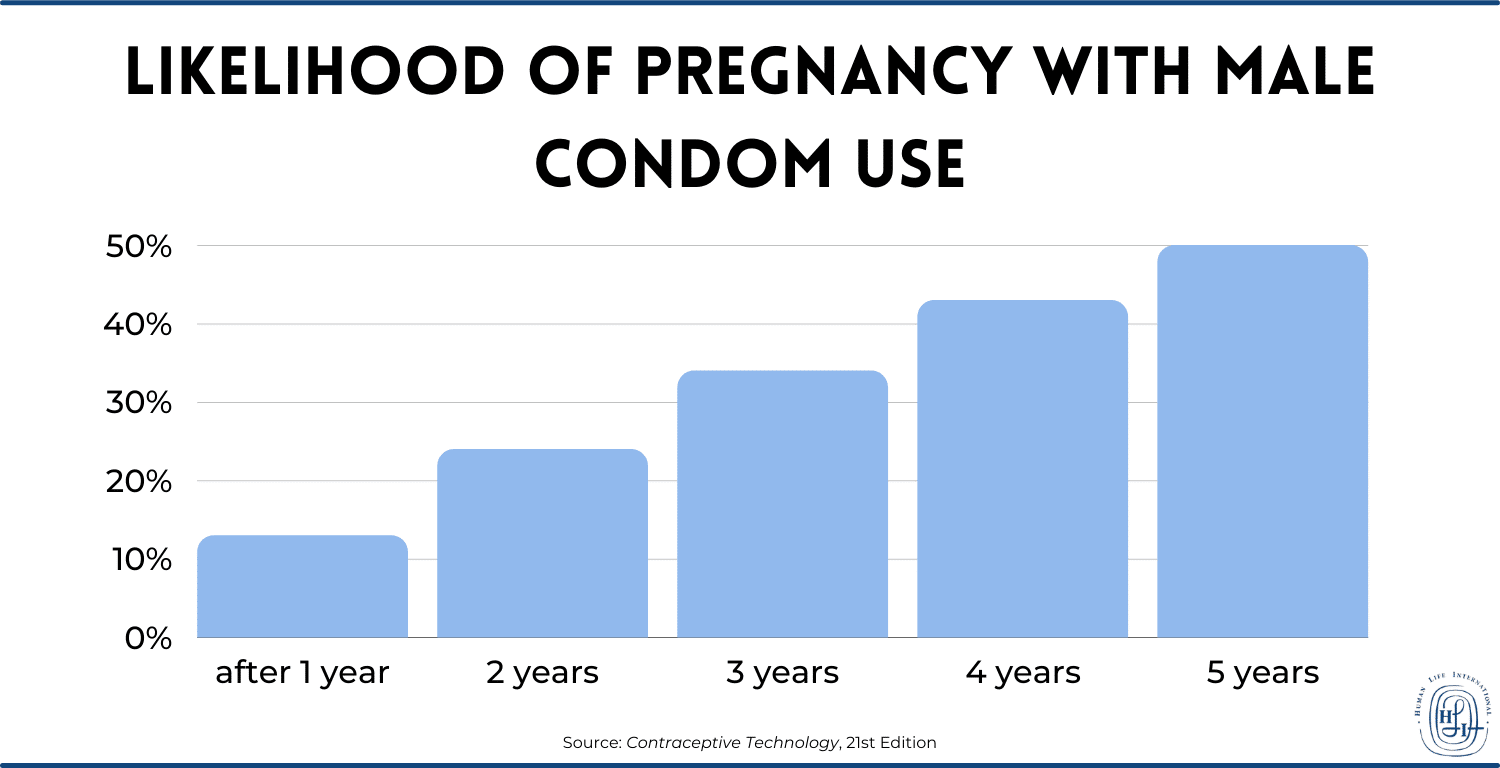
Within a year, 13% of sexually active women whose partners use condoms for contraception become pregnant, according to Contraceptive Technology, 21st Edition, and other top scientific sources. After two years, this means 24% have a pregnancy. After three years, it’s 34%. After four years, it’s 43%. After five years, it’s 50%.5
The bottom line: condoms don’t “prevent pregnancy” in the long run.
These figures are derived from studies of committed, adult couples using new and properly stored condoms which have not been allowed to degrade. The numbers for youth, for women with multiple partners, and for poor people and those in developing countries using expired or improperly stored condoms are likely worse.
This high “failure” rate means consistent leakage over time, inevitably making many episodes of sexual intercourse with condoms nearly equivalent to sex without condoms.
3. Condom Promoters Use Irrelevant Evidence
The United Nations Population Fund (UNFPA) and other global condom promoters claim that condoms have a 98% “success” rate, instead of the 87% “success rate[68]” documented in real-world studies.
The 98% success rate is based on ideal use every time by well-trained and highly disciplined adults under monitoring by scientists. What is relevant is the “success” rate of condoms by average people, who sometimes fail to put on condoms correctly or replace them immediately if the condom breaks in the heat of the moment, things that happen in the real world over time.
Even studies of trained, committed adult couples using new and properly stored condoms find a real-world “pregnancy prevention success” rate of 87% over a 12-month period (Contraceptive Technology, 21st Edition; same datum as above).6 Unmarried teenagers, often the targets of condom promoters, almost certainly have a far worse record.
4. Ultimately, Condoms Have Failed When Measured by National Statistics
Almost everyone is aware of the massive campaign to promote condom use that has gone on for decades around the world, including the free distribution of condoms by the millions through schools and health clinics in the United States and other Western countries. Obviously, it’s not working.
Teen pregnancy in the United States is still at sky-high levels (there were 171,674 births to mothers aged 15 to 19 in 2019, which of course does not count any pregnancies stopped by abortion or miscarriage, nor births to 10-to-14-year-olds7). There was a decline in teen pregnancies in recent years, probably due to a rise in either chastity or, more likely, other forms of contraception. Additionally, nearly 900,000 abortions are performed each year in the United States as of 2019 (the last year with data reported), a number that is down from previous years but still monumental.8 And given the massive numbers of STIs pervading the United States and the whole world[68], it’s a safe bet to say condoms haven’t worked for those either.
Conclusion
The main point of this article is that abstinence is important not only from a moral standpoint, but also from a basic scientific and health standpoint. Even disregarding the immorality of condoms for a moment, the fact remains that they can’t even do what they are supposed to do—especially not on the scale of a country’s population. They will not save anyone from the consequences of promiscuous indulgence.
[1] The formula used for this particular calculation was 1 – (1 – 0.0606)n, where n is the number of uses of the condom (so in this case, n=10). The original data is from Robert Hatcher et al., Contraceptive Technology (21st Edition; New York: Ayer Company, 2018), 100.
[2] Please contact HLI’s Dr. Brian Clowes, PhD, at bclowes@hli.org[70] to access the meta-analysis raw spreadsheet (F-21-07). It compiles the twenty-three studies’ data.
[3] S. A. Sanders, W. L. Yarber, E. L. Kaufman, et al., “Condom use errors and problems: A global view,” Sexual Health vol. 17, 9(1) (February 2012):81–95.
[4] Ibid.
[5] The “13%” datum is from Hatcher et al., Contraceptive Technology, 100. The formula for calculation of probability is the same as that used already above: 1 – (0.87)n, where n is the number of years (0.87 is the probability of not becoming pregnant in the first year, and so the second year needs a compounded probability, 0.872=0.7569, subtracted from 1; etc.).
[6] Hatcher et al., Contraceptive Technology, 100.
Posted By
HLI Staff
On
In
Contraceptives and Abortifacients |
No Comments
“Blessed are the wombs that never bore.”
The End of Generation
Sterilization is, in one sense, the epitome of anti-life activities, the crowning legacy of people like Margaret Sanger[73], Marie Stopes[74], and other eugenicists. This is because it fully achieves the end that those activists hoped for: removal of the generative capacities of human beings. Like neutering or spaying dogs, anti-lifers permanently destroy men’s and women’s reproductive organs in sterilization. The selling point is that it allows unregulated pleasure with absolutely no chance to beget new life. So, as a supposed permanent and absolute “alternative” to contraception, the purpose for most individuals who pursue sterilization is to allow pleasure without promise—no promise to bear life. However, the purpose of many ideologues who push sterilization around the world (especially in the Global South and developing countries of Africa and South/Southeast Asia) is more akin to eugenic population control, just like Sanger and Stopes originally intended.
With sterilization, fecundity is permanently canceled. Indeed, when Our Lord said that there would come days when they would call the barren blessed, He might have been thinking of our own time.
The topic of sterilization is broad. In this article, we will focus on technical and medical concerns for individuals who get sterilized. We will start with general facts about sterilization, then consider the methods, health effects, and other concerns involved with female sterilization and then male sterilization. But none of this should eclipse the main point about sterilization: it is inherently, unmitigatedly, grossly immoral[75]. To destroy organs of the human body with the direct intention of ending the capacity to beget children is directly repugnant to the first commandment of the Creator: “Be fruitful and multiply” (Gen. 1:28).
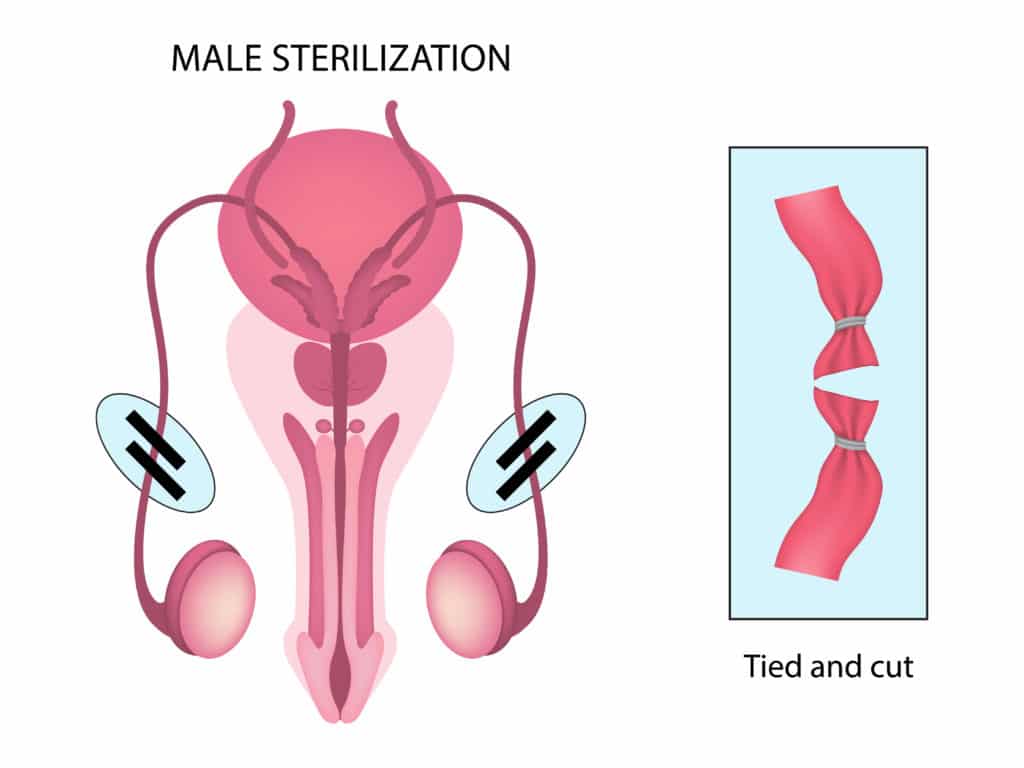
Male and Female Sterilization: General Facts
There are two halves of the coin: female sterilization and male sterilization. The former has historically been more popular, although the latter is rising in popularity, and efforts to push it are increasing. As methods of so-called “family planning,” both kinds of sterilization are a major part of the global population control campaign that has been targeting Africa, South Asia, and other regions of the world for decades. To this end, sterilization is usefully marketed as “permanent contraception,” and it is often administered immediately after a woman gives birth, for example in places like Kenya.1 It is also administered after abortions.
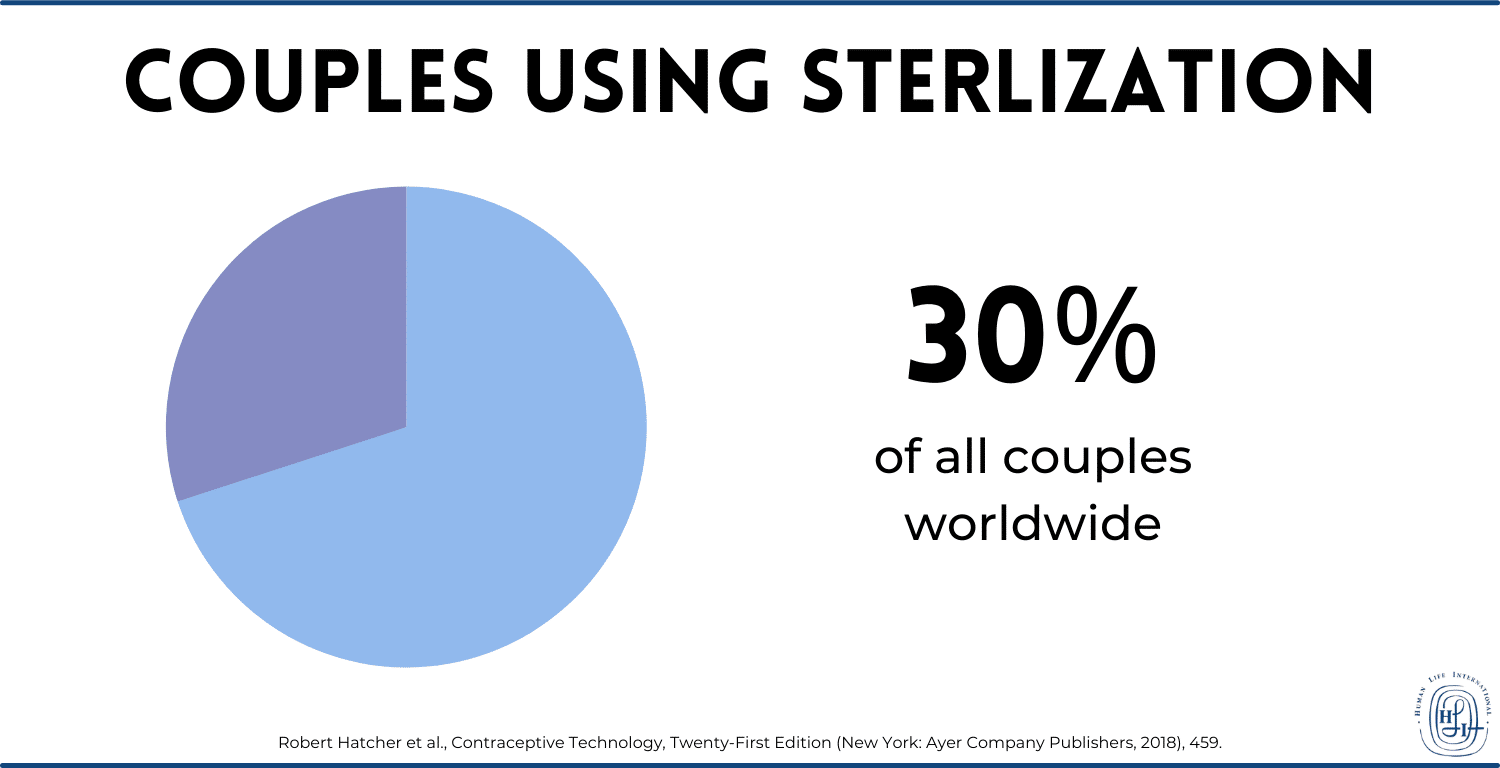
What may be most surprising about sterilization is that it is the most popular kind of “contraception” (as far as it can be considered a kind of contraception) in the United States, and it is very popular in other developed countries. According to Contraceptive Technology, 21st Edition, the 2011-2013 National Survey of Family Growth found that 25.1% of contracepting couples used female sterilization, and 8.3% used male sterilization. That gives a whopping 33.4% of couples using sterilization as their “method of choice” to prevent new life in their sex acts, or 12.5 million people—all in the United States alone.
Around the world, more than 30% of all couples use sterilization.2
These are enormous numbers, and even though only 10% of couples in the developing world are sterilized, Western ideologues would love to increase that number, since they would prefer those populations to have the least chance of producing new life.
With all that said, we will move onto the specifics of the procedures and damages done to women’s and men’s bodies in sterilization. Fair warning: sterilization is one of the most disgusting anti-life phenomena to talk about, so readers should beware. We must discuss not only the moral depravity of sterilization, but also some specific health risks associated with the methods of female sterilization and male sterilization; this requires some gory details.
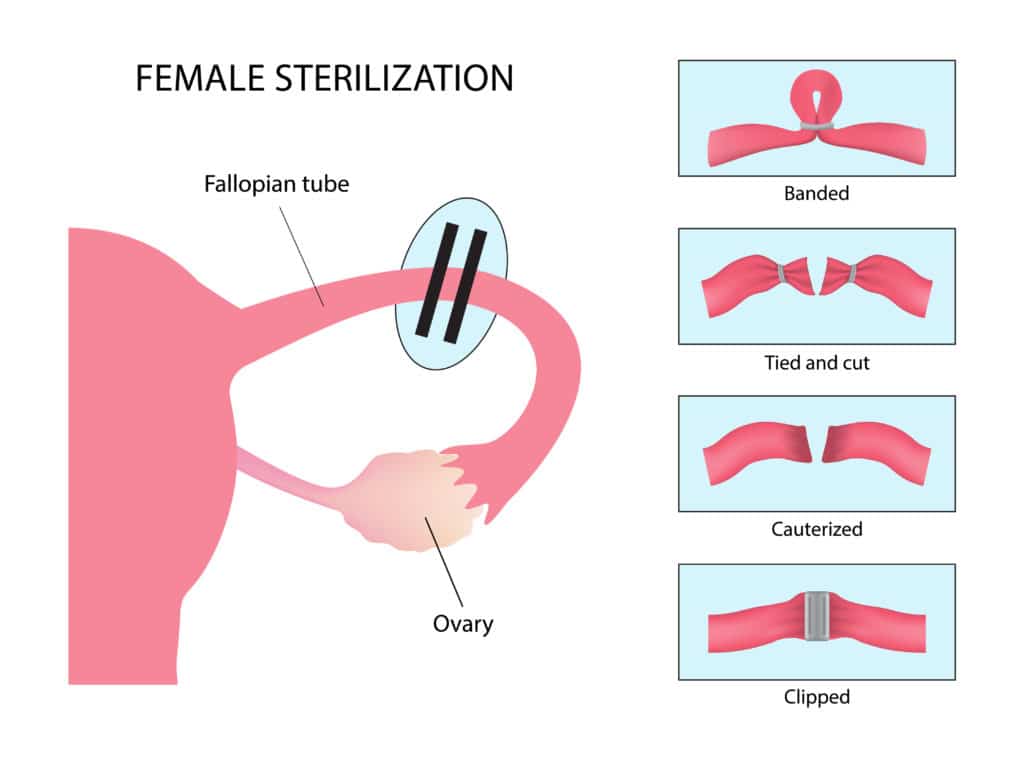
Female Sterilization (Tubal Occlusion, Ligation, or Removal)
Historically, female sterilization has been more popular than male sterilization. Female sterilization basically consists of destroying or somehow preventing the function of the fallopian tubes, which carry eggs from the ovaries to the uterus. If the tube has been damaged or removed, then eggs can’t pass through the tubes, and sperm cannot reach them during intercourse. There are various forms of tubal ligation, occlusion, or removal, in which the fallopian tubes are tied, cut, clamped, or even blocked according to diverse and grotesque techniques. Let’s discuss them.
All of the following information comes from Contraceptive Technology, 21st Edition, from Chapter 16 on so-called “Permanent Contraception” (i.e. sterilization).
Most tubal ligation/occlusion procedures are performed by laparoscopy, where a camera is inserted into the pelvic cavities via small incisions. Using this format, the surgeon has many choices as to the method of destroying or maiming the woman’s fallopian tubes, including:
Electrocoagulation – The surgeon uses electricity to burn and cauterize the fallopian tubes; tissue coagulates, blocking the passage of eggs.
Mechanical clips and bands – The surgeon can place various name-brand clips, rings and bands, like the Falope Ring, the Ulka-Clemens clip, and the Filshie clip, to squeeze the fallopian tubes shut. The devices are made of metal, plastic, or silicone, and can have spring parts and interlocking teeth.
Salpingectomy – Technically this method is neither tubal ligation nor occlusion, because instead of blocking or “tying” the tubes, the surgeon just cuts out the fallopian tubes entirely.
Minilaparotomy – The surgeon makes incisions below the navel, and from there can either perform a partial salpingectomy (cutting away the middle of the fallopian tube and leaving behind some behind on the ovary side and the uterine side) or a full salpingectomy.
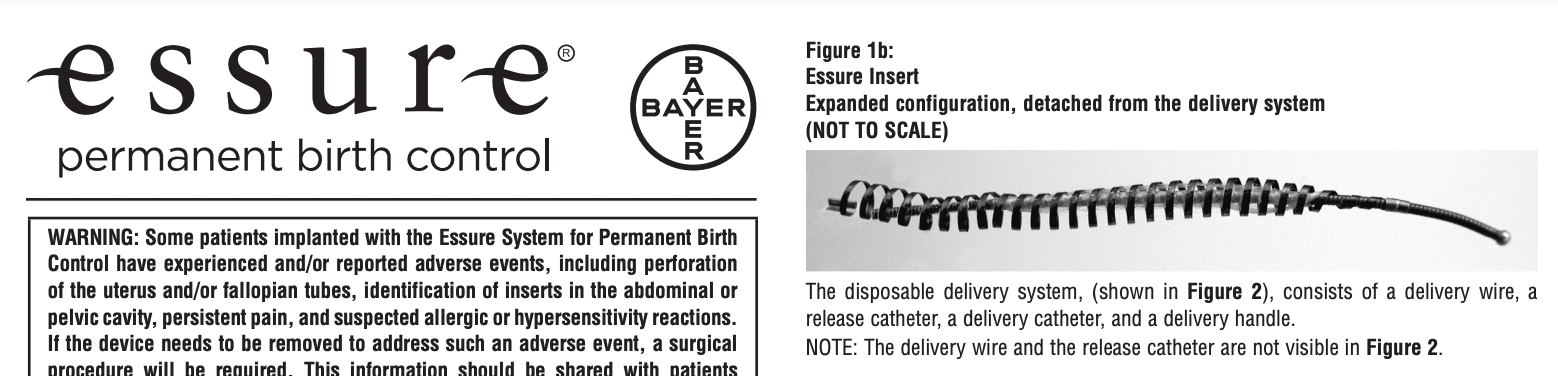
There is also the hysteroscopic approach, which inserts a camera through the cervix rather than through incisions in the abdomen. The only method available in the United States that uses the format is the Essure device, a metal coil inserted into the fallopian tubes. The device itself is meant to cause inflammation by embedding fibers into the wall of the fallopian tube, which will then develop inflamed tissue that eventually seals off the tube, after about three months.
Screenshot from the Essure Coil’s Instructions for Use
Health Effects of Tubal Sterilization
One of the consequences of allowing sharp instruments and metals inside one’s body in order to damage and destroy healthy organs is the range of potential side effects. Sterilization is inherently unhealthy, and the list of associated health risks is not short.
Menstrual Problems
Although menstrual problems are probably the least common health problems, some women do report them. There are not enough good randomized, controlled experiments on the subject to make any proper assertions (according to the authors of Contraceptive Technology), given that many women used hormonal contraceptives prior to being sterilized, and weight change and aging present confounding variables. But it seems to be the case that at least some women report menstrual problems, enough for there to be a named post-tubal ligation syndrome, although Contraceptive Technology doesn’t consider it definitive. Between 2% and 4% of patients in trials for Essure and Adiana (a different device, which is no longer in production) said they had menstrual disturbances following their procedures, which, again, some explain away by alluding to other possibilities.
What is known is that, at least subjectively, some women feel tubal sterilization affects their menstruation.
Surgical Complications
Laparoscopic surgery comes with the risk of bowel, bladder, and major vessel injuries. While these are not common, it is dependent on the conditions of the woman’s anatomy, including obesity, and the surgeon’s skill. But accidents can always happen; minor and major injuries are unpredictable and possible. Other complications, like the necessity for a blood transfusion and febrile morbidity (severe fever), occur 0.9% to 1.6% of the time. Contraceptive Technology also indicates the possibility of wound infection and prolonged pelvic pain. In hysteroscopic Essure placement, rupturing the tube occurs in 1% to 3% of cases. Infections, bleeding, and injury to other organs are also possible in hysteroscopic procedures.
Post-Ablation Tubal Sterilization Syndrome
In women who have received both tubal sterilization and endometrial ablation, or removal of the uterine lining (sometimes used to treat excessive uterine bleeding), the incidence of post-ablation tubal sterilization syndrome is 8% to 33%. The syndrome refers to the accumulation and distention of blood stuck in the cornua (where the fallopian tubes and the uterus meet) or the near end of the tube; the trapped blood causes significant pain. There is an increased risk for women who receive the Essure device and later need an endometrial ablation, because certain ablation procedures use radiofrequencies that can be conducted by the Essure’s steel core and damage other organs.
Chronic Pelvic Pain
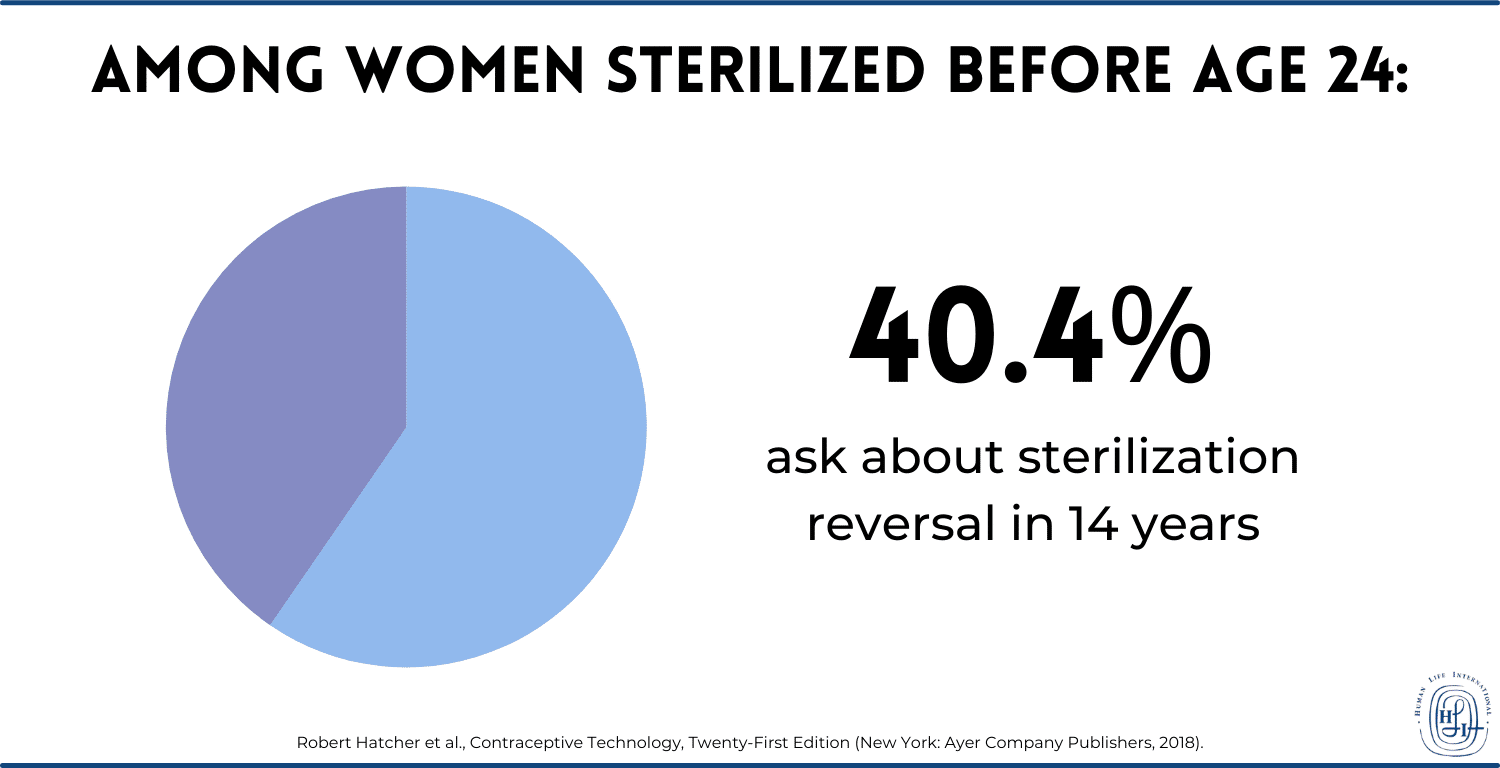
As with menstrual dysfunction, reports of chronic pelvic pain are difficult to analyze statistically. However, they do exist, especially among younger patients who have had previous menstrual trouble. According to a study cited in Contraceptive Technology, after Essure placement, 8.1% of women may have pelvic pain, continuing in 4.2% of them after three months. However, these numbers grow; within a year of placement, 19.2% of women report pelvic pain, and after a year, 30.8% do. This number is likely to increase with time, and the risk of pain increases with previous history of pelvic pain.
Hysterectomy
It is unknown why, but there is a high risk of the need for a hysterectomy, or the removal of the uterus, in women who have had tubal sterilization surgery. They can be up to 4.4 times as likely to receive the procedure than those couples whose male member had a vasectomy. The probability of getting a hysterectomy after 14 years from being sterilized was found to be 17%, quite a high probability for such a rare procedure.
Ectopic Pregnancy
The most frightening risk of any kind of tubal ligation/occlusion or removal, but especially electrocoagulation, is ectopic pregnancy. This is a pregnancy where the fertilized ovum implants in the fallopian tube, rather than the uterine wall. It is usually fatal for the woman if left untreated, since the baby will grow in the wrong spot and rupture the woman’s abdomen. There have been extremely few cases of babies who survived and were born from an ectopic pregnancy.
Now, the purpose of sterilization is to sterilize and render pregnancy impossible; but new life can still arise at times (we’ll get to that in a bit). When it does, the risk that the resulting pregnancy is ectopic is very high, about 30%—15 to 20 times the rate for non-sterilized women.3 The total cumulative probabilities over ten years for ectopic pregnancy for each method of tubal sterilization are still low, around 1% or less. But for women under thirty, the probability is greater; it can triple to about 3% (31.9 per 1000 sterilizations) after electrocoagulation in particular.
Other Major Concerns with Tubal Ligation/Occlusion or Removal
The problems with tubal sterilization do not stop at moral and health concerns; there are also practical concerns as well. For instance, although female sterilization is supposed to be permanent, there is remote potential for the method not to succeed in preventing new conception. As we mentioned, when that happens, an ectopic pregnancy is likely. The various methods carry different probabilities, but the average rate is 0.5% pregnancy within a year after tubal sterilization. Over five years, the cumulative rate ranges from 0.5% to 1%, and that number increases the younger the woman is when she gets sterilized. As for the Essure device, estimated rates are higher, 0.5% in one year and 1% over ten years. However, “successful placement rates” (meaning the metal coils are stuffed securely into a woman’s tubes) range from 81% to 98%, meaning there is greater likelihood that the coils won’t even be placed properly to prevent conception.
There’s an even bigger problem with sterilization: women regret it. As reported in Contraceptive Technology:
The cumulative fourteen-year probability of regret is 12.7%, or about one in eight women.
Women who were younger than thirty when they had their “tubes tied” regretted with a probability of 20.3%; that’s more than one in five young women. Even the rate for women older than thirty when operated on was 5.9%, over one in twenty women.
And within the same fourteen-year period, the rate of women who ask for information about reversing sterilization is 14.3% (about one in seven women). For women who get sterilized before age 24, the number can be as high as 40.4%.
That’s too bad, because reversal is extremely impractical; there is a reason they call it “permanent contraception” in the anti-life arena. If you want to become pregnant after female sterilization, either you have to use in-vitro fertilization, itself highly immoral, and highly expensive[76], or you try to reverse the operation. The reversal depends very specifically on each case and the method of tubal sterilization employed, but all attempts to reverse carry risks. These include surgical mishaps, anesthetic accidents, and ectopic pregnancy rates between 4% and 8%.
Lastly, there are a few things to note about the Essure device, which carries with it special concerns. Soon after its introduction, increasing numbers of women began to request its removal, for all kinds of reasons. These included pregnancies, chronic pelvic pain, menstrual dysfunction, and nickel hypersensitivity (not to mention improper placement of the coil itself). In November 2016, Essure was required to have a black box warning about the myriad problems it has.
Now let’s take a look at the male counterpart to female sterilization: vas sterilization.
Male Sterilization (Vas Sterilization or Vasectomy)
The mechanism of male sterilization is the severing or otherwise blocking of the vasa deferentia (plural of vas deferens), which prevents them from transmitting sperm from the testes. As a result, semen will have no sperm in it, and intercourse will be sterile. The most common way to do this is to snip the tubes as a form of very precise castration, but there are also newer ways to obstruct these delicate tubes. As with tubal sterilization for women, the various methods of male sterilization are quite disgusting; we will cover them for completeness’s sake, and to see just how grotesque the whole business of sterilization is.
Again, all of this information is from the sixteenth chapter of the twenty-first edition of Contraceptive Technology.
The first step to destroying the function of the vasa is to isolate them; this can be done in a variety of ways. Conventional vasectomy is the oldest method, which uses 1.5- to 3-centimeter-long incisions in the scrotum, made with a scalpel and sewn shut by suture after the sterilization is done. The actual sterilization occurs when the vasa are cut and occluded using surgical scissors, and then the ends of the sliced tubes are occluded (using one of the methods described in the next paragraph). “No-scalpel vasectomy” was invented in 1974 by a Chinese doctor looking for a faster way to do this. First, a ring clamp is placed around the vas, perivasal tissue (tissue around the vas), and the skin of the scrotum. Then a special “vas dissector” is used to aid in grasping the vas, snipping it, and occluding the ends according to the various methods. Sutures are not used normally, since only a tiny incision is made. No-scalpel vasectomy is a type of so-called “minimally invasive vasectomy,” which includes various other technical variants of manipulating and maiming a man’s private parts.
After that, there are various methods of occluding or ligating or removing the vasa deferentia, including:
Ligation – The surgeon ties up the tips of the snipped vasa deferentia using ligatures, removing about a centimeter from each vas between the tied ends.
Clips – Similar to ligation, but the surgeon uses clips to clamp the sliced ends shut instead of ligatures.
Thermal or electocautery – The surgeon uses electrical or thermal instruments to burn the mucosa around the snipped ends of each vas.
Fascial interposition – The surgeon usually uses this method in addition to others; a layer of spermatic fascia, which is connective tissue nearby the vas, to add an extra barrier between one or both ends of the split vas.
The Marie Stopes International technique – The surgeon uses electrocautery to burn and destroy two and a half to three centimeters of each vas; this method is the only one that does not involve division or excision of any part of the vasa. It is not used in the United States, but only in countries where MSI operates, many of which are poor developing countries.
There is also chemical occlusion, but this is a very uncommon method for humans.4 That’s just one more indication that sterilization is like neutering or spaying a dog.
Side Effects of Vas Sterilization
As with female sterilization, male sterilization carries with it a retinue of health detriments, stemming from the very fact that any kind of sterilization is directly contrary to health, which is the proper functioning of the body. It is inherently unhealthy, and that shows. While the list of potential side effects of male (vas) sterilization is slightly shorter than that of female (tubal) sterilization, it does not mean there is necessarily a smaller rate for some of them. Nor does it mean that they are any more pleasant.
Surgical Complications
While vasectomy is less invasive than tubal sterilization, there is always the possibility of complications, including severe ones. There can be injuries from slicing instruments, or the procedure can go awry in various ways:
One particularly difficult possibility is that the same vas deferens is occluded in two places, rather than both vasa deferentia. This both invalidates the procedure and can cause more damage (that is, more than what the inherently damaging operation already does). It is a mistake made more likely by using a “single midline incision” in no-scalpel vasectomies (i.e. instead of two).
Although there are only 0.5 deaths per hundred thousand men sterilized by vasectomy, 1% to 2% of men who get sterilized do form hematomas (bleeding inside of the scrotum) or get infections, regardless of the method used.
Fournier’s gangrene, a condition in which flesh decays under a serious infection, has also been reported, though very rarely.
In general, while under 3% of vas sterilization procedures result in medical need, the list of possible complications, in addition to the above, can include: vasovagal reaction (slowing of the heart and blood flow that can result in faintness and more),5 lidocaine poisoning (too much anesthetic), bleeding, bruising, and swelling.
Chronic Scrotal Pain
One of the most unpleasant possible side effects of vasectomy is chronic scrotal pain, which afflicts between 1% to 2% of men who get sterilized. This pain can be severe, so much so that it has its own name: post-vasectomy pain syndrome. It can take months or years to show up, and when it does, it can become a continual health problem. While its source is unknown, speculation includes all manner of difficulties, from congestion of the occluded vasa, to explosion of the epididymis (the intermediate tube between the testicle and the vas deferens), to damage to the scrotal or spermatic cord nerves. In cases where regular treatment fails, surgery might be required, including various excisions, all the way to orchiectomy (removal of the testicals from within the scrotum).
Anti-Sperm Antibodies
One other special difficulty that comes from vas sterilization is the formation of anti-sperm antibodies. While only 8% to 21% of men in the general population have anti-sperm antibodies, an incredible 50% to 80% of sterilized men have them. While these antibodies, which kill sperm, are not otherwise dangerous to the body, they matter in two cases:
Sterilization “failure” (i.e. regular operation of the reproductive system that results in pregnancy)
A reversal attempt
With that, then, let’s move on to discuss these cases.
Other Major Concerns
While we shouldn’t consider impregnation a “failure” of a system designed to do just that, the male sterilization procedure, just like the female one, can still allow for pregnancy (meaning its anti-generation function isn’t foolproof). Vas sterilization generally will allow pregnancy 0.15% of the time (as opposed to 0.5% for tubal surgery), which makes it a more “effective” anti-generation method. But pregnancies still can happen. And the cumulative probabilities of pregnancy per 1000 vasectomies is: after one year, 7.4, and after two, three, and five years, 11.3.
But the real concern, as with female sterilization, is the possibility of regret. Permanently damaging himself and destroying his fertility is inherently a regrettable decision for a man. Rates of overall regret among men are 1% to 2%, which is lower than that of sterilized women. However, the women in men’s lives regret the vasectomy at rates of 6% to 8%. Like with tubal sterilization, the younger or more uncertain a man’s relationship future is, the higher the likelihood of regretting the permanent decision to neuter himself.
And that decision, again like tubal sterilization, really is essentially permanent. There are only two tenuous options after a vasectomy:
In-vitro fertilization or other “assisted reproductive technologies”—in other words, expensive, artificial, and highly immoral technological parodies of intercourse
An attempt at reversal, which involves extremely technical and advanced microsurgical skills on the part of the operator.
The second method’s impracticality makes sense when one considers that two tiny tubes have been sliced, blocked, tied, or otherwise maimed, and now they have to be reconnected. In addition, timing becomes a serious factor in an attempt at reversal. If a reversal attempt is performed within ten years after a vasectomy, rates are somewhat better; after that, rates of impregnations drop off to less than 50%. If a man wanted to get a woman pregnant, even after reversal, anti-sperm antibodies could have an enduring effect that likely hinders or altogether arrests the possibility of conception. In general, post-reversal pregnancy rates range from 38% to 89%, while IVF rates are 17% to 36%.
In short, “permanent contraception” describes vas sterilization accurately in the sense of permanence. Fair warning to men who would castrate themselves.
The “Choice” That Ends Choice
Everyone has the freedom to make medical choices that affect his or her health. However, many people are not aware of the damage that sterilization inflicts on their bodies in the long run. Others feel that the risks are outweighed by the seductive but false promises of freedom and security that sterilization offers in the short term.
The fact of the matter is that anyone who chooses sterilization is forced to accept hard realities:
You are forced to accept risks to your health. The side effects of various medical procedures of tubal occlusion/ligation and vas surgery vary from minor inconveniences to fatal difficulties. All side effects are unpredictable. If you choose a sterilization procedure, you are exposed to health risks that you cannot predict or avoid and potentially cannot treat
You can never change your mind. The moment you have a sterilization procedure, you give up choice in the matter forever. Although reversal procedures are possible, they are expensive and likely unsuccessful. You may even be led down a compoundedly immoral path by attempting IVF, which is gravely sinful[76], as well as expensive and not necessarily successful. For all intents and purposes, then, you will never have the option to bring forth a child if your circumstances or views change.
The end result is that sterilization, by inflicting severe damage to a body, removes a person’s control over both parental capability and health. It is simply and objectively the destruction of one’s reproductive organs. The medical advice that sterilization is a “safer choice” for “contraception” is contradictory, since the methods of sterilization inherently require administering damage to a previously healthy body and setting its future safety at serious risk. And furthermore, rather than protecting a person’s ability to lead a healthy life, they limit his or her options by permanently removing fertility, for all intents and purposes rendering him or her incapable of ever becoming a mother or a father.
Sterilization, rather than providing the promised freedom and safety, restricts a person to a condition of uncertain personal health and irreversible infertility. But the bottom line is that these natural problems are the reflection of supernatural problems. The reason sterilization and its consequences are so horrific to discuss is because they are morally egregious. Sterilization is certainly a mortal sin, and its practical permanence is one of the reasons it is worse than contraception. Not only is it intended to inhibit God’s life-giving intent for human sexuality simply for the purpose of lust, but it also directly destroys His creation, the male or female body.
We urge you to explore our other resources that discuss the beauty of human sexuality[69] as God intended it: between one man and one woman, open to life, for all their life.
+ Endnotes
[1] Faith Kasiva, Robbed of Choice: Forced and Coerced Sterilization Experiences of Women Living with HIV in Kenya, edited by Jane Godia (African Gender and Media Initiative, 2012).
[2] Robert Hatcher et al., Contraceptive Technology, Twenty-First Edition (New York: Ayer Company Publishers, 2018), 459.
[4] V. P. Dixit, N. K. Lohiya, M. Arya, and M. Agrawal, “The Effects of Chemical Occlusion of Vas Deferens on the Testicular Function of Dog: A Preliminary Study,” Acta Eur Fertil, December 1975, vol. 6(4): 348–53, https://pubmed.ncbi.nlm.nih.gov/1217450/[78].
[5] J. J. van Lieshout, W. Wieling, J. M. Karemaker, and D. L. Eckberg, “The Vasovagal Response,” Clinical Science 81, no. 5 (November 1991): 575–86, https://pubmed.ncbi.nlm.nih.gov/1661644/[79].
Abortifacient Brief: The Intrauterine Device
Posted By
Brian Clowes, PhD
On
In
Contraceptives and Abortifacients |
8 Comments
The intrauterine device (IUD) is a foreign body inserted into the uterus. IUDs are made of a non-reactive plastic such as polyethylene and may include active chemicals or elements such as progesterone or copper which slowly diffuse into the uterus over a period of several years.
The intrauterine device has several contraceptive (non-abortive) effects:
It prevents sperm from fertilizing ova
It releases ions that interfere with fertilization
It thickens the cervical mucus
It inhibits sperm capabilities
These are all purely contraceptive effects.
But IUDs also irritate the endometrium (the lining of the uterus) and make it inhospitable to the blastocyst (the very early developing human being), which is an abortifacient effect[16].1
Nearly half a century ago, the American Medical Association recognized that “the action of the IUDs would seem to be a simple local phenomenon. That these devices prevent nidation [implantation] of an already fertilized ovum has been accepted as the most likely mechanism of action.”2 The Food and Drug Administration (FDA) concurred in this assessment, finding that “IUDs seem to interfere in some manner with the implantation of the fertilized egg in the lining of the uterine cavity. The IUD does not prevent ovulation.”3
Nothing has changed. The patient information pamphlets for all of the IUDs made today describe in detail this abortifacient action. For example, the PIP for the Skyla IUD says that one of its mechanisms of action is “alteration of the endometrium.”
In summary, every IUD ever manufactured prevents implantation, meaning that they are all abortifacients.
These devices ensure that the uterus is as barren and hostile to new life as a desert. In fact, this abortifacient action is so efficient that scientists recommending the IUD for “emergency contraception” note that only one in 1,100 women will remain pregnant after inserting the device from two days to two weeks after their last unprotected intercourse.4
Controversy over the IUD
The first modern-day IUD, the Grafenberg Ring, was placed on the market in 1915. Several other companies immediately saw the opportunity for profit, and by the mid-1930s, there was a proliferation of IUDs for sale. They sported intimidating names such as the Sterilette, the Collar-Button, the Wishbone, the Silkworm Pust, and the Star.
Some of the devices were of good quality, but many were made of “cheaper, noncorrosive metals, or of celluloid, bakelite, and chromium-plated metals rather than gold.”5
According to one expert at the time, “Sometimes these [cheaper IUDs] were claimed to be made of solid gold in order to enhance the price, and a few practitioners took economic advantage of the need and ignorance of women.”6
More than 70 different types of IUDs have been manufactured over the last century. Some of these have consisted of polyethylene with barium sulfate so they could be detected by X-rays. The Dalkon Shield, which was the most popular IUD in use for several years in the United States, was of this type. It was withdrawn from the market in 1984 due to a number of maternal deaths.7
Other IUDs, including the Progesterone-T, were loaded with varying doses of progesterone crystals that were usually suspended in silicone oil. This IUD released about 24 milligrams of progesterone a year. It was originally promoted under the truly Orwellian label “Uterine Therapeutic System.”8
The copper IUDs (including the “Copper-7,” “Copper-T” and “Tatum-T”) discharged from 50 to 75 micrograms of ionic copper into the uterus each day. These copper ions interfere with the life-sustaining functions that regulate implantation of the new human life in the uterus. Copper has been proven to be the active agent in these IUDs because identical devices are ineffective without the element. Each copper IUD is effective at causing early abortions for about four years.9
There are five IUDs currently [in 2022] available on the American market:
The first type is the non-hormonal Copper T 380A (ParaGard), which consists of a flexible T-shape containing copper collars on both arms and a copper coil along the stem and is supposedly good for up to ten years of sterility.
The second type of IUD is loaded with a total of 52 milligrams of levenorgestrel (LNG an artificial progestin) and releases it at a rate of about 20 micrograms per day, declining to 14 micrograms per day after five years.10Liletta and Mirena are in this class of IUD.
The third type is the lower-dose IUDs, which have 13.5 to 19.5 milligrams of levenorgestrel and are effective for about three years. The Skyla and Kyleena IUDs are in this class.
Complications Associated with IUD Use
According to their patient information pamphlets, complications associated with the IUDs in current use include:
sterility
hemorrhage
perforation of the uterus, colon, bladder, or small or large intestine
cervical lacerations
cervical dysplasia (developmental abnormalities)
deep embedding of the IUD (a serious problem in developing countries, where women may have had the devices in their uteri for a decade or more)
fragmentation of the IUD
development of hydatidiform moles
salpingitis (inflammation of the uterine tubes)
pelvic inflammatory disease (PID, which often leads to infertility or sterility)
This is nothing new. Until about 1960, the medical community generally condemned IUDs because of their severe side effects. Alan Guttmacher, former President of the Planned Parenthood Federation of America, said in 1959, “Intrauterine devices are mentioned only to be thoroughly condemned because of their ineffectiveness, their potential source for infection and irritation, as well as their carcinogenic potential.”11
Although IUD technology had not advanced in the slightest, the entire medical community performed an abrupt about-face in the mid-1960s and began to accept the device. But serious complications were documented almost immediately. In 1974, the FDA summarized complaints received about the various IUDs on the market at that time.
The FDA had received reports of 238 cases of spontaneous septic abortion from women who had become pregnant with IUDs in place. Of these women, 21 died. The Dalkon Shield was involved in 14 of these deaths and 209 cases of septic abortion, and the Lippes Loop caused 5 deaths and 21 septic abortions.12
Overall, there were about 15,000 IUD-related hospitalizations annually in the early 1970s.13
A.H. Robin Pharmaceuticals made the Dalkon Shield IUD from 1971 to 1974. Documented reports of severe injuries began to surface almost immediately after initial distribution, and on 29 June 1975, the FDA announced it intended to “require special warning notices for users of the intrauterine devices, the contraceptives that were linked to 43 deaths in recent years.”14
A.H. Robin pulled the Dalkon Shield from the market in 1975. By 1985, 13,000 women had sued the company for damages relating to sterility, miscarriages and pelvic infections. Incredibly, some population controllers, including Stephen Mumford and Elton Kessel ― who peddle the dangerous sterilizing chemical quinacrine in developing countries ― have tried to sanitize the image of the Dalkon Shield so that it can make a comeback.15
Ortho Pharmaceuticals withdrew its Lippes Loop from the American market in 1985, and G.D. Searle withdrew its Copper-7 and Tatum-T IUDs in 1986 when its liability insurance lapsed. Searle also faced 775 lawsuits from women who suffered injuries from their IUDs or who conceived babies with birth defects when the devices did not work properly.
Because of widespread negative publicity, only 1% of women using birth control were on the IUD by 1995, but this number had risen to about 9% by 2017.16
Why Is This Abortifacient Called a Contraceptive?
When discussing abortifacient means of birth control, the “family planners” call us pro-lifers “anti-science” when we claim that the IUD causes early abortions. They say that human life begins at implantation, not fertilization.
But there is no logical reason to make this claim. What is the difference between the early human being (blastocyst) the hour before it implants and the hour after?
Whenever there is such confusion, we may find the answer in the dishonest manipulation of terminology by the “family planners.”
In 1963, the United States Department of Health, Education and Welfare (HEW) defined “abortion” as “all the measures which impair the viability of the zygote at any time between the instant of fertilization and the completion of labor.”17
Until the mid-1960s, scientists universally acknowledged that conception happened at the moment of fertilization of the ovum by the spermatozoa somewhere in the Fallopian tube. But pro-abortionists and population controllers already had their sights set on a shift from contraceptive to abortifacient methods of birth prevention, and abortifacient research was already ongoing in Japan and several European countries.
To make abortifacients acceptable to women, and to circumvent laws designed to prohibit abortion, the “family planners” realized that they had to blur the line between contraceptive and abortifacient action.
They could do this only by changing the definition of “conception” from fertilization [union of spermatozoa and ovum] to implantation. Under the new definition of “conception,” if a device or drug ― such as an IUD or Depo-Provera ― prevents implantation, then no abortion takes place. Under the new definition, abortion would only occur if a chemical or device killed a preborn child who had already implanted in the endometrium (lining) of the uterus.
The pro-abortionists’ continuing agitation for a change in terminology finally bore fruit in 1965, when the American College of Obstetrics and Gynecology (ACOG) published its first Terminology Bulletin, stating, “Conception is the implantation of a fertilized ovum.” This semantic subterfuge resulted in the Bulletin inventing two misleading terms for early abortion: “Post-conceptive contraception” and “post-conceptive fertility control.”18
The deception by the medical establishment regarding the definition of “conception” coincided exactly with its devaluation of the preborn child. Neither change in attitude nor terminology was based upon some revolutionary discovery in medical technology or knowledge: the changes were made purely to further the anti-life goals of the medical profession and the pro-abortionists.
The IUD and Population Control
IUDs have confronted the anti-fertility industry with a number of forbidding problems, the greatest of which was the proven danger of the devices. This did not stop the IUD manufacturers from turning a tidy profit by dumping their products on the poor women of developing countries.19
Despite being faced with an avalanche of lawsuits claiming damage from its Copper-7 and Tatum-T IUDs, Searle said that it would continue to make IUDs for women in developing countries under population control programs funded by the United States and other Western countries.20 This is yet another example of the West’s “contraceptive imperialism[81]” ― a willingness to dump unsafe and even lethal products on poor women of the developing world after judging them to be too risky for Western women.
Health risks associated with IUDs are a serious matter with grave implications that are not immediately evident. All of the IUDs currently on the market have patient information pamphlets that warn about the possibility of uterine perforation, especially among women with unusually-shaped uteri, or among women who have IUDs inserted immediately after childbearing. This shows that IUDs are especially ill-suited for use in developing countries, where anemia and malnutrition are often endemic, especially among women and children.21
Naturally, long-acting birth control that women cannot control is ideal for use by coercive governments[82]. For three decades, right up to the alleged end of its dreaded “one-child” program, nearly half of all Chinese women of childbearing age had IUDs implanted after their first birth because the only alternative the government gave them was immediate sterilization.22
Final Thoughts
The IUD is the perfect example of nature’s lack of tolerance for abuse. The very idea of having a piece of plastic or metal inserted into the body in order to cripple a healthy reproductive system should be repugnant to women, but the anti-life mentality has advanced so far that millions of women are willing to risk the consequences.
+ Endnotes
[1] Robert A. Hatcher, M.D., M.P.H. Contraceptive Technology [New York City, Ardent Media] (20th Edition, 2011). Chapter 7, “Intrauterine Contraceptives (IUCs), pages 147 to 192.
To look up the patient information pamphlets (PIPs) for all intrauterine devices (or for any drug, for that matter), visit the National Institute for Health’s DailyMed archives[40]. The latest PIPs for the currently manufactured brands of IUD are Kyleena (July 2021), Liletta (April 2020), Mirena (August 2021), Paragard T 380A (September 2019), and Skyla (July 2021). All of these patient information pamphlets confirm that IUDs sometimes act by altering the endometrium, thus making implantation either impossible or much more difficult. This is an abortifacient effect.
[2] American Medical Association Committee on Human Reproduction. “Evaluation of Intrauterine Contraceptive Devices,” Journal of the American Medical Association, February 27, 1967, page 155.
[3] United States Food and Drug Administration. “Text of Required Patient Information for IUDs.” Federal Register, May 10, 1977.
[4] Kelly Cleland, Haoping Zhu, Norman Goldstuck, Linan Cheng and James Trussell. “The Efficacy of Intrauterine Devices for Emergency Contraception: A Systematic Review of 35 Years of Experience.” Human Reproduction, May 8, 2012.
[5] Norman E. Hines, Ph.D. Practical Birth-Control Methods [New York City: Viking Press, 1938], page 138.
[6] Norman E. Hines, Ph.D. Practical Birth-Control Methods [New York City: Viking Press, 1938], page 138.
[7] Rainey Horwitz. “The Dalkon Shield[83].” The Embryo Project Encyclopedia, January 1, 2018.
[8] E.B. Connell. “The Uterine Therapeutic System: A New Approach to Female Contraception.” Contemporary OB/GYN, June 1975, pages 49 to 55.
[9] H.J. Tatum. “The New Contraceptive: Copper Bearing IUDs.” Contemporary Obstetrics and Gynecology, January 1973, pages 61 to 63.
[10] Robert A. Hatcher, M.D., M.P.H. Contraceptive Technology [New York City, Ardent Media] (20th Edition, 2011). Chapter 7, “Intrauterine Contraceptives (IUCs), pages 147 to 192.
[11] Harold Dubrow, M.D., and Alan Guttmacher, M.D. “The Present Status of Contraception.” Mt. Sinai Journal, 26:118-124. 1959.
[12] “The Dalkon Shield and the Questions of Safety.” Medical World News, September 13, 1974, pages 58 to 61. Also see Catherine Breslin. “Day of Reckoning.” Ms. Magazine, June 1989, pages 46 to 52. This article describes the inside story of the Dalkon Shield disaster.
[13] H.S. Kahn and C.W. Tyler. “IUD-Related Hospitalizations: United States and Puerto Rico, 1973.” Journal of the American Medical Association. 234:53-56(1973).
[14] “American Public Health Association Launches Campaign to Save IUD.” ALL News, March 9, 1987.
[15] S.D. Mumford and E. Kessel. “Was the Dalkon Shield a Safe and Effective Intrauterine Device? The Conflict between Case-Control and Clinical Trial Study Findings.” Fertility and Sterility, June 1992, pages 1,151 to 1,176.
[17] Public Health Service leaflet No. 1066, United States Department of Health, Education and Welfare [HEW], 1963, page 27.
[18] American College of Obstetrics and Gynecology (ACOG). Terminology Bulletin, “Terms Used in Reference to the Fetus” [Chicago: ACOG], September 1965.
[19] Filipino women have probably suffered more abuse from American and European pharmaceutical companies than the women of any other nation, and this is recognized in the Filipino press. For example, one article stated that, “Many drugs and devices which are not even permitted in the United States have found their way to Manila where they are dumped on hapless Filipino women. One example was the IUD (or intrauterine device) which is associated with a great deal of disease and despair” [Max Ricketts, Mabuhay Times, April 16-29, 1991, page 12].
The Philippines is one of several nations where I have personal experience with first-world “contraceptive imperialism.” When I visited Davao City in 1995, the population suppression effort was in full swing. Propaganda posters promoting “family planning” were painted on schoolyard walls, usually prominently featuring a Catholic priest, to give the false impression that the Church supports contraception. On October 22, I visited a little shed where the Dominican sisters near Davao City perform medical procedures. These religious sisters, who are also qualified as medical doctors, pulled intrauterine devices out of women all day every Tuesday. In the late 1980s, an international population control group conducted a “Safe Motherhood Initiative” in the rural areas surrounding Davao City. They offered to give free pelvic examinations to all women between the ages of 15 to 44. While doing so, they secretly inserted IUDs into all of them! Some villages in this area therefore have no children at all under the age of about seven. As the sign on the shed door indicated, the sisters pull IUDs out of women for 25 pesos (about one dollar). If they do not have the money, they do not have to pay. Often the sister/doctor must work for a long time to remove them because the Dalkon Shields or other IUDs have embedded themselves deeply in the wall of the uterus.
[20] Front Line Updates. “Searle Removes IUDs from U.S. Market.” NRL News, February 27, 1986, page 4.
[21] Uterine perforation is one of the complications listed in the patient information pamphlets for Kyleena (July 2021); Liletta (April 2020); Mirena (August 2021); Paragard T 380A (September 2019); and Skyla (July 2021).
[22] Sui-Lee Wee. “After One-Child Policy, Outrage at China’s Offer to Remove IUDs.” The New York Times, January 7, 2017.
Abortifacient Brief: Implants
Posted By
Susan Ciancio
On
In
Contraceptives and Abortifacients |
4 Comments
Since the Supreme Court ruled on the legalization of birth control, millions of women—often oblivious to its dangers[45]—have used one of its many forms. Manufacturers make billions[85] off a woman’s desire to have sex with little to no consequences. While the pill is the most popular type, other methods continually entice women. Birth control implants are one such method.
A birth control implant is a device, about the size of a matchstick, used to prevent or impede pregnancy. A doctor inserts this device just under the skin of a woman’s inner upper arm. Usually containing levonogestrel, the implant releases this chemical into the woman’s body daily for years at a time.
Birth control implants are marketed as an easy solution to the “problem” of fertility. Women can have them inserted and then forget about them. This eliminates forgetfulness or user error. And it increases efficacy. But these implants have had a far-from-smooth introduction into the market. In addition, they do not prevent against STDs.
It all began with a device called Norplant. Norplant was first developed and approved abroad in the 1980s. But it wasn’t until 1990 that the FDA approved[86] its use in America. Norplant was made of silicone and contained six capsules[87] containing levonorgestrel. It was effective for up to five years.
Soon after Norplant was introduced, women found themselves facing health crises.
Side Effects of Norplant
Almost immediately, women began experiencing terrible side effects. These included[88]:
severe headaches
anxiety and panic attacks
depression
acne
weight gain of 60 to 100 pounds
excess growth or loss of hair
ovarian cysts
breast pain
skin discoloration
infection at the implant site or numbness in the arm
a variety of menstrual disorders
These side effects were so harmful that over 36,000 women joined a class action lawsuit[89] against American Home Products Corporation, the parent company of the maker of Norplant. The plaintiffs claimed that the company “misled customers about the severity of Norplant’s side effects.” In 1999, American Home settled without admitting any wrongdoing. The company agreed to pay more than $50 million total. The settlement gave each woman slightly under $1,500.
According to a lawyer for the women who sued the manufacturer, the most severe side effects that he knew of were “enlarged ovaries and fallopian tubes that burst, causing the need for hysterectomies and/or the removal of the tubes and ovaries.”
Following the class action lawsuit and public outcry, the distributor withdrew Norplant[87] from the US market in 2002. Its production was discontinued worldwide in 2008.
But like a phoenix rising after its death, birth control implants would not stay dead long.
In came Jadelle—an FDA-approved implant that is only marketed overseas.
Jadelle
While Norplant had 6 matchstick-sized implants, Jadelle is a set of two. Each contains 75 mg of levonorgestrel.
Like Norplant, a doctor must insert the rods—one at a time—into the woman’s arm. The doctor uses a local anesthetic and makes the incision. Often, swelling, bruising, or discoloration result at the site. Some women report pain or itching. In addition, some women have had skin reactions such as blistering, tingling, numbness, or scarring.
According to RX List[90]: “Immediately after insertion[91] of Jadelle® . . . implants, a low continuous dose of the hormone is released into your body. Pregnancy is prevented by stopping ovulation (so eggs will not be produced regularly), and thickening the cervical mucus (making it more difficult for the sperm to reach the egg). There may also be other effects that contribute to pregnancy prevention.”
Abortifacient Effects
It doesn’t mention these “other effects[92].” But we know what they are. Jadelle—and other similar hormonal contraceptives—alters the lining of the endometrium to prevent implantation of a fertilized egg. That means that a baby has already been created. However, that baby is unable to attach to the wall of the endometrium to continue to grow. Because he cannot attach, he dies.
These three methods combine to give Jadelle a less than 1% failure rate.
Jadelle is effective for up to five years. If the woman weighs over 132 lbs, her doctor may recommend that she have the implant removed after the 4th year. This is done to maintain its efficacy.
Side Effects
No hormonal contraceptive comes without side effects. And Jadelle has many. About 10% of women suffer from[93]:
Between 1 and 10% of women suffer more serious side effects. Some of these include:
Chest pain
Depression
Asthma
Fatigue
Palpitations
Bronchitis
Ovarian cysts
In addition, according to the Jadelle pamphlet[94], a woman may experience an allergic reaction to the device. Some of these reactions include:
shortness of breath
wheezing or difficulty breathing
swelling of the face, lips, tongue, or other parts of the body
rash, itching, or hives
The pamphlet also warns: “You may have a higher risk of an ectopic pregnancy if you get pregnant while your implants are in place. An ectopic pregnancy can be a serious and life-threatening condition. It can also cause problems that may make it harder for you to become pregnant in the future.”
Not only is the implant potentially deadly for a woman’s baby, but it’s potentially deadly for her as well.
Hormonal contraceptives can cause fatal blood clotting
How Are Birth Control Implants Removed?
Just as a woman must have a doctor insert the device, so must she return to the doctor to have it removed. While this is supposed to be an easy procedure, it is not always.
The overall incidence of removal difficulties in the clinical trials, including damage to the implants, was 7.5%. If removal of the implant(s) proves difficult, close the incision and bandage the wound, and have the patient return for another visit. The remaining implant(s) will be easier to remove after the area is healed. It may be appropriate to seek consultation or provide referral for patients in whom initial attempts at implant removal prove difficult.
So while many women have an easy time with the removal of the implant, a significant number of women experience difficulty. That difficulty has not gone unnoticed by the manufacturer.
Enter a new kind of device. This one is detectable on an x-ray.
Implanon and Nexplanon
Jadelle is not available in the US. So, in 2006, the FDA approved Implanon[87]. Implanon was a single thin rod produced by a division of Merck that released etonogestrel. Its improved design made it easier to insert and remove.
However, just four years later, Merck replaced Implanon with Nexplanon[96]. Nexplanon was designed to be visible through an x-ray, which makes it easier to find and remove. It also comes with an improved insertion device.
Nexplanon is currently the only available birth control implant in the US. The FDA has approved it for up to three years[87]. Unlike Jadelle, which may not be as effective in women over 132 lbs, Nexplanon isn’t contraindicated in overweight women. Yet the information pamphlet also states that the device may lose its effectiveness in women with a BMI greater than 30.
Just like the other birth control implants, Nexplanon has a fewer than 1%[96] failure rate. And its side effects are similar to those of its predecessors.
Cysts may develop on the ovaries and usually go away without treatment, but sometimes surgery is needed to remove them.
Besides changes in menstrual bleeding patterns, other common side effects reported in women using Nexplanon include: headaches; vaginitis (inflammation of the vagina); weight gain; acne; breast pain; viral infection such as sore throats or flu-like symptoms; stomach pain; painful periods; mood swings, nervousness, or depressed mood; back pain; nausea; dizziness; pain and pain at the site of insertion. Implants have been reported to be found in a blood vessel, including a blood vessel in the lung.
Again, we see significant dangers to women. Sadly, many women feel that the gains outweigh the pains.
Who Uses Birth Control Implants, And Where Do They Get Them?
According to the Kaiser Family Foundation[87]: “In 2015-2017, the most recent years for which there are national data, about 4% of women ages 15-44 who currently use contraception used the implant.”
Those who use birth control implants tend to be younger women and women from low-income households. Many have Medicaid or are uninsured.
Researchers believe that women from these backgrounds prefer the implant because of its ease and because they want to prevent pregnancy for a longer period of time.
The Kaiser Family Foundation also reported the results of a 2016-2017 survey of obstetricians. This survey found that almost three out of four OBGYNs who provide obstetrical care offer the implant. Those who don’t offer it were asked why. They cited reasons such as lack of interest and the fact that their staff were not trained to insert it.
That brings us to another issue with birth control implants. Staff need special training to insert it. The FDA requires a two-hour, in-person training from the manufacturer. While the cost of the training is free, travel to the site and any other expenses incurred are the responsibility of the trainee. Some doctors don’t feel that it’s worth the effort.
Many low-income women use federally qualified health centers. However, because of the cost of the birth control implants, oftentimes these facilities do not stock them. Furthermore, their staff do not have the training. A 2017 study found that just over two-thirds of these facilities carry implants, Meanwhile, about 98% of Planned Parenthood clinics carry them. In addition, Planned Parenthood clinics allow a woman to come in for just one visit to have the birth control implants inserted. Some health centers require the woman to have an initial appointment and then return for the insertion.
Punitive Use?
When Norplant was still available in the US, it caused controversy for another reason. Judges in several cases made its use a requirement or part of a plea deal[98] for women who had been accused of child abuse or endangerment.
According to Hastings Constitutional Law Quarterly[98]: “Within months of its approval, several judges around the country had already succumbed to Norplant’s allure. In California, Nebraska, and Texas, judges imposed use of Norplant as a mandatory condition of probation for mothers convicted of child abuse….Elected officials, judges, and other interested parties began advocating and implementing widespread and sometimes mandatory use of Norplant, often as a means to fight poverty.”
Initially, officials targeted women using drugs. Their hope was that Norplant would prevent them from creating babies who suffered from addiction at birth. Sometimes Norplant was used as an incentive. If the woman agreed to using it, she would get something in return. And finally, it was used as a condition of probation for mothers who were convicted of child abuse.
But was this ethical? Is it morally right to coerce a woman to have chemicals inserted into her body?
Right to Privacy?
According to Hastings Constitutional Law Quarterly[98], “The United States and California Constitutions provide a right to privacy that protects decisions regarding procreation, parenting, and medical treatment from government intrusion.”
The Constitution provides no explicit right to privacy. However, the Supreme Court has found what it terms as a “zone of privacy.” It first ruled on this in 1965 in Griswold v. Connecticut[99].
This right to privacy has been extended to include a person’s right to refuse “unwanted medical treatment and other invasions of bodily integrity.” Further, the Court allows a person to refuse medical treatment in a criminal setting as well.
The courts quickly realized that women could not be forced to undergo any kind of medical procedure. And that included birth control implants.
The Catholic Church is adamant about maintaining bodily integrity because the body is a temple of the Holy Spirit. As HLI’s Brian Clowes states[75]: “Any mutilation of the body—including extreme ‘body modifications’…and attempts to cripple it for social reasons (including sterilization)—is to be condemned. Such mutilations ‘violate the integrity of the human person.’ Direct sterilization destroys the normal and proper functioning of a body system and is thus illicit in all cases.”
While birth control implants aren’t sterilization, they do destroy the normal and proper functioning of the human body for years at a time. In addition, forcing a woman to undergo this treatment is an offense against her dignity as a human being.
Final Thoughts
Advertisements, organizations, and social media all paint a joyous picture of the freedom that women can experience while using birth control implants. Rarely will they acknowledge that this “freedom” comes at a cost.
Isn’t it time that women exercise true freedom? Isn’t it time they listen to the facts? The facts paint a very different picture. Yet the facts tell the truth. Hormonal birth control, including implants, is detrimental[45] to a woman’s health. And sometimes they kill a baby.
Women, you only get one body. Treat it with respect.
The Truth about Emergency Contraception
Posted By
Brian Clowes, PhD
On
In
Contraceptives and Abortifacients |
No Comments
What Is Emergency Contraception?
Even with all of the different contraceptives and abortifacients on the market today, women forget to use their birth control, think their birth control method might have failed, or were coerced into sex.
Many of these women resort to “emergency contraception,” a term that covers several drugs or devices that are used after intercourse (instead of before) to avoid pregnancy. EC can take several forms[100]. The most common are:
The morning-after pill (MAP)
Doubling up on birth control pills
Insertion of the Copper-T, or ParaGard intrauterine device.
The abortion drug mifepristone (RU-486) can also be used as emergency contraception.
Other drugs, including Meloxicam, Indocin and Ranitidin (normally used for pain, inflammation control and acid reflux, respectively) are under investigation for potential use as emergency contraception.
To begin with, the very term “emergency contraception” is inaccurate. It is another attempt to erase the distinction between true contraceptive and abortifacient action[16]. When pro-lifers hear terms like “emergency postcoital contraception,” they can be sure that what is being discussed is an abortifacient cocktail.
1. Morning-After Pills
The term “morning-after pill” is also a misnomer, since these methods are most effective when used immediately after intercourse. There are three types of MAP:1
Those that use the same hormones (estrogen and progestin) that are used in standard birth control pills, but in higher doses. These are specifically intended to be taken after intercourse instead of before, and are available without a prescription to anyone 17 years of age or older. Wyeth’s Ovral is the only MAP of this type, and consists of four tablets containing both the progestin norgestrel and synthetic estrogen in the form of ethinyl estradiol.
Progestin-only (levonorgestrel) pills, known by the brand names Plan B and its generic equivalent Next Choice. These contain either a single 1.5 mg dose of LNG or two doses of 0.75 mg LNG each, taken 12 hours apart within 72 hours of intercourse. Barr Laboratories’ patient information insert for Plan B says that its product “… may inhibit implantation (by altering the endometrium). It is not effective once the process of implantation has begun.”
Anti-progestin pills. These go by the brand names Duprisal 30, ella, ellaOne, Ulapristal 30 and UPRIS, and contain ulipristal acetate. They are available by prescription only and are effective for up to five days after intercourse.
2. Doubling Up on Birth Control Pills
The second type of emergency contraception consists of taking several doses of standard combined birth control pills that contain both progestins and synthetic estrogen. The Food and Drug Administration has determined that 26 brands of birth control pill, including Alesse, Levlen, Lo/Ovral Nordette, Ovral, Tri-Levlen and Triphasil are safe for use in what is sometimes called the “Yuzpe Regimen.”
3. IUDs
Finally, there are the IUDs. Paragard is the only non-hormonal copper intrauterine device used in the United States today. It releases copper ions that are toxic to both gametes (sperm and ovum) and decreases the probability of fertilization. The copper ions are also toxic[101] to the very early embryo, either killing it or preventing it from implanting. Paragard can be inserted up to five days after intercourse to prevent a continuing pregnancy.
All forms of emergency contraception are abortifacient in nature. This is clearly specified on all of the patient information leaflets issued by their manufacturers. However, the mainstream media can always be depended upon to deliver misinformation to the public. For example, the New York Times has claimed,[102] “Studies have not established that emergency contraceptive pills prevent fertilized eggs from implanting in the womb, leading scientists say.”
Since the medical profession switched the definition of “conception” from fertilization to implantation in the mid-1960s for the sole purpose of paving the way for new abortifacients, doctors do not believe they are misleading the public when they claim that “emergency contraception” does not cause abortions. Contraceptive Technology Update states, “MAP does not cause an abortion … RU 486 is different from MAP as it us used later and causes an already implanted ovum/embryo to detach from the uterine lining, which is why it has been called the “abortion pill”” [emphasis in original].1
The population control group Academy for Educational Development used the tried-and-true tactic of promising us the moon and the stars when it said, “Because almost half of all unintended pregnancies in the United States end in abortion, EC could therefore eliminate half of all abortions. … Using ECPs within 5 days of unprotected sex cannot result in abortion because pregnancy has not begun. And again, if ECPs are taken after implantation, the pregnancy will not be interrupted.”2
Catholicism and Emergency Contraception
Questions have arisen as to whether Catholic hospitals should administer emergency contraception to rape victims.
On this topic, the United States Conference of Catholic Bishops has written[103]:
A female who has been raped should be able to defend herself against a potential conception from the sexual assault. If, after appropriate testing, there is no evidence that conception has occurred already, she may be treated with medications that would prevent ovulation, sperm capacitation, or fertilization. It is not permissible, however, to initiate or to recommend treatments that have as their purpose or direct effect the removal, destruction, or interference with the implantation of a fertilized ovum.
In other words, Catholic doctors may administer a medication to rape victims that has a contraceptive, but not an abortifacient, effect.
The problem here is that we cannot know for certain whether or not a woman who has been raped has already conceived. Current available technology in the form of pregnancy tests, including luteinizing hormone protocols and ovulation tests, cannot reliably provide this information after fertilization and before implantation. They can only inform us that implantation has taken place. By then, of course, emergency contraception would not work to end the pregnancy.
We have seen that all abortifacient methods (including all forms of emergency contraception) have multiple mechanisms of action, as clearly defined in Paragraph 12.1 of the standardized “Highlights of Prescribing Information” forms required by the Food and Drug Administration. One of these modes of action is alteration of the endometrium, thus making implantation impossible or difficult. In fact, no birth control drug exists that has a purely contraceptive mode of action. Therefore, whenever these pills are taken, or a Copper-T IUD is inserted after sexual activity, there is a significant risk that a new human life will be destroyed.
One of the necessities of good moral judgment is good scientific facts. If the facts are in doubt, then the safest course of action must conform only to the verifiable facts. In this case, when uncertainty injects itself, the safest course of action must be taken, even if this means doing nothing.
This principle led to the Pontifical Academy for Life issuing an October 2000 statement[104] that stated, “From the ethical standpoint, the same absolute unlawfulness of abortifacient procedures also applies to distributing, prescribing and taking the morning-after pill. All who, whether sharing the intention or not, directly cooperate with this procedure, are also morally responsible for it.”
Conclusion
We should therefore treat the abortifacient Plan B “morning-after pill” and so-called “emergency contraception” in the same manner as we would handle Depo-Provera, the birth control pill (OC), Norplant and the intrauterine device (IUD). All of these work a certain percentage of the time to end the life of the early developing human being and are therefore inadmissible.
Theologian Father Peter Damian Fehlner, North American Superior for the Franciscan Friars of the Immaculate from 1996 to 2002, clarified this point. He said[105] that as long as there is doubt as to whether or EC is abortive, it may not be used. “The fact is, if we have any doubt about whether a given action would directly risk someone’s life, entail a violation of justice or threaten the salvation of a soul, we may not act on the basis of a scientific probability. That means even if the pill in Plan B is only ‘dubiously’ abortive, we simply may not use it at all.”3
+ Endnotes
[1] “Ask Your Clinician… ” Contraceptive Technology Update, November 1995, page 141.
[2] Academy for Educational Development. “Building Emergency Contraception Awareness Among Adolescents: A Toolkit for Schools and Community-Based Organizations.” 2003, page 8. Others have made the same promise; see Mary Ann Marshall. “Morning Becomes Prophylactic.” Ms. Magazine, August/September 1999, pages 40 and 41.
[3] For an in-depth discussion of EC administration to rape victims at Catholic hospitals, see “Scientific Certitude, Moral Certitude, and Plan B.” The National Catholic Bioethics Quarterly, Winter 2011, pages 7 to 11. Also see Human Life International’s Truth and Charity Forum. “When in Doubt, Choose Life[106].”